
52 足と足首の痛み Foot and Ankle Pain

Firestein & Kelley's Textbook of Rheumatology, Eleventh Edition シリーズ、52章は足と足首の痛み。
キーポイント
足関節痛の鑑別診断はたくさん上がるが、症状から解剖学的部位を特定できれば鑑別の幅はかなり狭まる。
身体所見では、足と足首のほとんどの構造は皮下であるため触診が容易である。
非手術的治療法には、装具、靴、理学療法などがある。
足関節外科の手術のほとんどは、人工関節置換術、矯正骨切り術、骨切除術、腱剥離術および腱移行術、滑膜切除術のいずれかに分類される。手術を検討する際には、術後の松葉杖などの約束事を徹底できるか、軟部組織や血管に問題がないことが重要な要素となる要素となる。
医学的管理の進歩により、以前は関節置換術が必要であった多くの炎症性関節炎患者において、関節温存手術が可能となった。
はじめに
・足部および足関節の痛みは、中高年者の約5人に1人が罹患している。
・そのうち、2分の1から3分の1が日常生活に支障をきたしているが、関節リウマチ以外で日常生活に支障をきたすことはほとんどない。
・足と足首の痛みは女性に多く、原因の多くは靴にある。
・足関節痛の鑑別診断は多岐にわたり、腱、靭帯、筋、骨、関節、関節周囲構造、神経、血管の障害、および関連痛が含まれる。
・足関節の痛みの最も一般的な原因のひとつは、変形性関節症(OA)で、好発部位は外反母趾、中足部、足首である。
・足首は複雑な関節で、捻挫、骨折、軟骨損傷などよく傷害を受ける関節であるが、股関節や膝関節など他の体重を支える関節に比べると障害の程度は軽い。
・足関節炎で原因が特定できないことはほとんどない。
・足関節OAの一般的な原因は、骨折や靭帯損傷などの外傷である。その他の原因としては、力学的な異常(扁平足やハイアーチ(凹足): 足の甲が極端に高い足)や、稀ではあるがヘモクロマトーシスのような全身疾患がある。
関節リウマチについて
・足関節痛は、新規発症の関節リウマチ(RA)の約15%から20%、すでにRAと診断されている患者では90%以上に認められる。
・医師は詳細な病歴聴取と身体診察から関節リウマチの足病変の評価を始めるべきである。
・レントゲン写真やCT、MRIなどの画像診断は、足関節の病態の評価に有用である。
・初期の非手術的治療には、内科的管理、理学療法、靴の修正、装具がある。
・難治性の症状に対しては、外科的治療が必要となる。ほとんどの外科手術は、関節固定術、人工関節置換術、矯正骨切り術、骨切除術、滑膜切除術(関節または腱)のいずれかに分類される。
身体診察
①歩行分析:患者が診察室に入るとき、足と足首の徹底的な歩行分析からはじめるべきである。The physician should begin a thorough physical examination of the foot and ankle with gait analysis, even if by simply observing the patient enter the examination room.
Pearl:人間の正常な歩行は、 立脚相と遊脚相(the stance phase, the swing phase)の2つの相に分けられる。
Comment: Normal human gait is divided into two phases. The stance phase is the weight-bearing portion of the gait cycle and comprises roughly 60% of normal walking. This phase begins with heel-strike and then extends through foot-flat to toe-off motion. Meanwhile, the swing phase of gait extends from toe-off to heel-strike and comprises the remaining 40% of the gait cycle.

・人間の正常な歩行は2つの相に分けられる。
・立脚相は歩行サイクルで足が地面に接地している間で、通常の歩行の約60%を占める。この相は、踵をつく動作から始まり、足を平らにしてつま先を離す動作までをいう。
・遊脚相は地面から足が離れている局面であり、歩行サイクルの残りの40%を占める。
・足、足首関節の診察のスタートは歩行を診察することです。右足がついていれば(立脚相)、左足は離れています(遊脚相)。
・立脚相、遊脚相のバランスはいろんな状況で変化します。歩行速度が増加してくると一般的には遊脚期の時間が減少します。痛みがあれば、患側の立脚相は短くなり、健側の脚に負担がかかります。
②視診:歩行分析のあとは患者の座位と立位で足と足首を診察します。After gait analysis, the physician inspects the foot and ankle, both with the patient in the sitting and standing position.
・RAでよくみられる変形は、外反母趾(bunion)、ハンマートゥ(Hammertoe: つちゆび)、扁平足、リウマチ結節である。Bunionって発音したくなる可愛い呼び名ですね。
Hammertoe: つちゆびは第2趾(ときに3趾、4趾)がZ字型に曲がり簡単に伸ばせなくなっている状態。外反母趾に第2趾ハンマートゥは合併しやすい(下図の左の通り)。


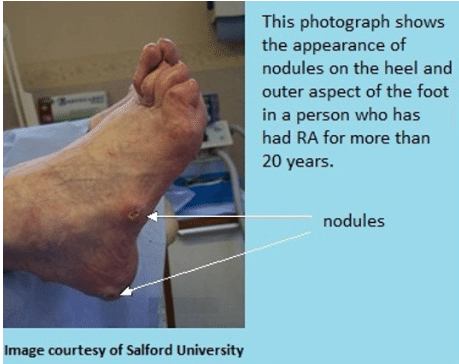
Pearl:リウマチ結節は足底のどこにでも発生しうるが、繰り返し外傷を受ける場所、例えば靴底からの刺激部位に多く認められる。
Comment: Rheumatoid nodules can appear anywhere on the foot but are often found in areas of repetitive trauma (i.e., at the site of irrita- tion from a tight shoe counter).
・リウマチ結節は物理的な刺激を受けやすい部位にでき、好発部位は肘、前腕伸展部、指、アキレス腱。
・足で刺激が受けやすい場所は、アキレス腱上、踵の後ろ、骨が盛り上がった部位(nodule)の上です。下の写真は分かりやすいです。
Pearl:靴のすり減りパターンにもチェックする
Comment: Finally, wear patterns on shoes should also be noted. As Hoppenfeld observed: “A deformed foot can deform any good shoe; in fact, in many cases the shoe is a literal showcase for certain disorders.- Physical examination of the spine and extremities, Norwalk, Conn, 1976, Appleton and Lange.
・Hoppenfeld曰く、変形した足はどんなよい靴でも変形させることができる。
・靴裏が、外側や内側が減っている、中心が減っている左右非対称に減っている、などからどのような足の変形が起きているか推測できるようです。ここはちょっと深掘りしてみましょう。
Wear Patterns on Your Shoes Tell a Tale- 靴のパターンが物語るものとは?

・正常:正常の靴のかかと部分の減り方は外側45°。中央ではなく後ろ外側45°….知らなかった。
・O脚:この正常角度よりも外側が減っていたらO脚。中足部も外側が減ります。
・X脚:正常角度より内側が減っていたらX脚、中足部も内側が減ります。
・扁平足:中足部は内側がすり減るのがポイントです。かかと部分は重症度に比例して内側が減っていきます。
その他いろいろ分かるようです
・一側だけすり減り:足の長さの違いや歩行の乱れ、骨格の不均衡
・外反母趾: 靴の幅が狭ければ靴の外側を圧迫する。
・ハンマートゥ:つま先の靴の上に隆起が現れる(下も圧迫しそう)、などなど
③ROM:足の可動域を評価する。足関節の受動的可動域は通常、背屈10~20度(上向き)、底屈40~50度(下向き)。後足部の正常な内反・外反はそれぞれ約20度と10度。第1MTP関節の「底屈」(屈曲)は約45度、「背屈」(伸展)は70~90度。After inspection of the foot and ankle, the physician performs range-of-motion analysis. Passive range of motion of the ankle is normally between 10 and 20 degrees of dorsiflexion and 40 and 50 degrees of plantarflexion. Normal hindfoot inversion and ever- sion are approximately 20 and 10 degrees, respectively. The first MTP joint should have approximately 45 degrees of “plantarflex- ion” (flexion) and 70 to 90 degrees of “dorsiflexion” (extension).

④触診:次に足と足首を徹底的に触診する。Next, the physician thoroughly palpates the foot and ankle.
Pearl: 足と足首の背面(上側)にはほとんど筋肉がない。
comment:The dorsum of the foot and ankle has little overlying musculature. As such, many of the bones and tendons are immediately subcutaneous and a great deal of information can be gained from palpating these structures.
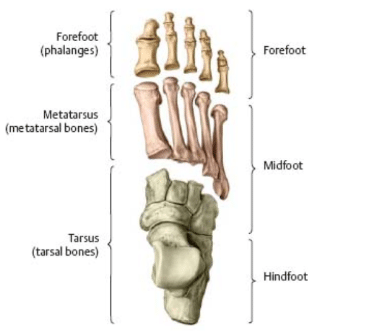
・そのため骨や腱がすぐ皮下にあるためしっかり触診することができる。前足部(forefoot)、中足部(Midfoot)、後足部(hindfoot: ハインドフット)、足関節の前後を丁寧に触診していく
各部位に生じる足の問題
・Forefoot 前足部:関節炎、外反母趾、ハンマートゥ
・Midfoot 中足部:関節炎、ストレス骨折、骨壊死(舟状骨)
・Hindfoot 後足部:関節炎、足底筋膜炎、ストレス骨折、内反足変形
Pearl: 足関節の評価の主役はX線写真である
Comment: Despite the abundant availability of advanced imaging modali- ties such as MRI and CT, radiographs remain the imaging main- stay in the evaluation of foot and ankle pain. Standard images consist of weight-bearing antero- posterior, lateral, and oblique views of the foot and anteroposterior, mortise, and lateral views of the ankle.
・足関節の評価の主役は、MRIやCTではなくレントゲンである。
・撮影方法:荷重をかけた状態で、①足正面・側面、斜位、②足首の正面、側面、Mortise(内旋位)。
・Mortiseとは「下腿を15-20内旋して」撮影する、らしいですがあまり聞いたことがないです。専門家はやっているんでしょうか?。
the leg rotated internally 15° to 20°, thus aligning the intermalleolar line parallel to the detector
Mortiseの狙いは次の通り-This projection is the most pertinent for assessing the articulation of the tibial plafond and two malleoli with the talar dome, otherwise known as the mortise joint of the ankle… つまり、遠位脛腓関節(脛骨と腓骨の間の下側)、脛骨と距骨、腓骨と脛骨の間が見えやすい。
https://radiopaedia.org/articles/ankle-weight-bearing-mortise-view

MRI
・RA初期でもMRIで滑膜炎、腱鞘炎、関節周囲の浮腫などを評価することができますが、個人的にはほとんど使用していません。
治療
①手術以外の治療:RAの治療の基本は抗リウマチ薬、ときどきステロイド。
Pearl: 靴の改良は患者に大きなメリットをもたらすことが多い
Comment: Shoes should be examined in the clinic to be sure that they can accommodate a patient’s deformity. Patients often feel best in shoes with a deep, wide toe-box, a firm heel counter, and soft heel. Well-constructed walking or jogging shoes usually pro- vide sufficient room for mild to moderate deformities. It is helpful to provide patients with a list of suitable manufacturers when making such recommendations.
・つま先が深く、幅が広く、踵がしっかりしてい柔らかいものが良い。よくできたウォーキングシューズやジョギングシューズであれば、軽度から中程度の変形には対応できる。おすすめのメーカーリストを提示すること。
・
外反母趾の160名が選ぶ!おすすめの靴・スニーカー10選!選び方も紹介、なんてサイトもありました。
https://sneakers-labo.com/sneakers-gaihanboshi/
・安めであれば無印良品(疲れにくいスニーカー )、かっこよさを求めればニューバランス996かスタンスミス。スタンスミスはもっていますが確かに、つま先が深く幅も広く、踵はしっかりしていて固くないきがします。
・さらに変形が強い場合は、靴の中敷きの調整もしてもらいます。
・装具もいろいろありますが、軟らかい素材のものが使いやすいと思います。外反母趾の装具は市販されているので試してもらっています。
永幡先生に、「ドクターショール ジェル インソール」がいいと教えてもらいました。
https://amzn.asia/d/g1ZoH4I
②手術療法
・変形が進み保存療法では痛みが抑えきれない場合、手術療法の適応となります。
RAの手術適応となる変形:外反母趾、開張足(横アーチの消失)、扁平足、外反(アライメント異常)
Pearl: 手術を行う大前提は、①手術部位の軟部組織や血管の問題がない、②術後のレジメン(松葉杖の使用や、体重をかけないこと)を遵守できるかどうか、である。
Comment: Two important factors must be taken into account when deciding whether or not to proceed with surgery. First, the soft tissues and vascular status must be carefully assessed. Both may be compromised and could negatively affect outcome. Second, the ability of patients to comply with the post- operative regimen (e.g., the ability to use crutches and not bear weight if necessary) must be considered. Even limited noncompli- ance can lead to a poor outcome, especially in fusion surgery.
・特に固定術ではしっかり安静を守れないと予後不良になる。
・手術部位が感染していたり、血流障害があると当然手術はできない。
・手術は関節固定術、人工関節置換術、関節形成術(矯正骨切り術、骨切除術)、滑膜切除術、のいずれかに分類される。
足関節の手術は、①関節固定術、②人工関節手術、の2つ。
足趾の手術は、①関節形成術、②人工関節手術、③関節固定術のなかから選択される。
Myth: 外反母趾の手術の第一選択は関節固定術である。
Reality: Previously, patients with RA and concomitant pes planovalgus or hallux valgus underwent fusion surgery. However, with advances in medical management of the disease, it is not unreasonable to attempt joint preservation surgery in patients who have mild to moderate disease, healthy soft tissues, and flexible deformities.
・以前は固定術を受けていたが、近年の内科治療の進歩により、変形が中程度であれば関節温存手術を試みるのがよい。
・このように現在は、MTPを温存する足趾形成術が主流になりつつある。
以上、なかなか深掘りすることのないDAS28で見落とされる足と足首について、でした。Kelleyはやはりいいですね。
この記事が気に入ったらサポートをしてみませんか?