Explanation of “Measures against clusters” at the Expert Meeting: The last hope for dealing with the new corona virus

The original article written by Kohei Yoshimine, laywer
20/03/2020 9:38pm
The infectious epidemic of COVID19 in Wuhan led to an rapid outbreak in Europe and the United States, and there seems to be no end to it. In Japan, there has been no explosive spread (expert meetings call it "overshoot") like in Wuhan, Europe and the United States, but it is still in a dangerous tightrope situation.
Currently, the center of measures against coronavirus in Japan is the expert meeting and cluster measures group of the Ministry of Health, Labor and Welfare. Both organizations seem to have top scientists and plan and implement the effective strategies-"cluster measures." Perhaps, the cluster measures are the last hope for Japan to survive this catastrophe while avoiding the social collapse, but it does not seem to preveil enough public announcement, thus its full picture remains unknown to everybody.
In this article, as I am a lawyer, not a medical expert, I will explain the actual and theoretical basis of cluster measures that I have understood by reading publicly available materials (especially materials from expert meetings and press conferences, notes by Prof. Minato Nakazawa). My target readers were assumed to have considerable background knowledge, but you may be able to understand without much trouble. However, please search for 𝑅₀ (basic number of reproduction) or COVID-19 symptoms on your own.
Index
1. At least 100,000 people die if failed
2. Rationale for cluster measures
3. Successful cluster measures
4. Cluster detection and "time difference of one month round trip"
5. Can "invisible clusters" be detected by reinforced inspection?
6. What we do
Reference
1. At least 100,000 people die if failed
(1) What happens when overshoot (infection explosion) occurs
Infection control strategies can be broadly divided into the containment (Suppression) and mitigation (Mitigation).
Generally speaking, if containment fails, the infection spreads exponentially and eventually ends with the acquisition of collective immunity. Collective immunity means that a certain percentage of the population becomes infected and gains immunity, so that the infection does not spread further within the population. The percentage of individual immunity required for collective immunity is determined by 𝑅₀, with COVID19 case estimated to be 40-70%.
Already containment failed for SARS-CoV-2
In this case, the theory is that the spread of the new corona is unavoidable, and it will eventually have to calm down to acquire collective immunity (at least to mitigate that damage). However, some people have made odd claims that despite containment failures, there is a way to avoid the spread of infection. That is the Experts Meeting / Cluster Countermeasures Group, whose claim is "Containment by Cluster Countermeasures". This is a strange strategy based on the strange nature of the new corona virus, and should be called "semi-containment." First, let's take a look at how much sacrifice will occur before reaching collective immunity.
First, let me try to calculate it myself.
If Japan's population is 100 million and 40% infected, 40 million are the patients. Of the 40 million people, 20% = 8 million are severely affected and 5% = 2 million are seriously ill. The number of hospital beds in Japan is 1.6 million, which is usually 80% or 90% occupied, so we cannot meet this demand at all. The estimated fatality rate of infected persons is 0.6-0.3%, so a minimum of 120,000 deaths. In Wuhan, the mortality rate is 3.8%, which means that the mortality rate jumps 10 times above the capacity of medical institutions. In that case, 3% would result in 1.2 million deaths.
Now let's take a look at some more realistic estimates. Here is the latest expert conference materials.
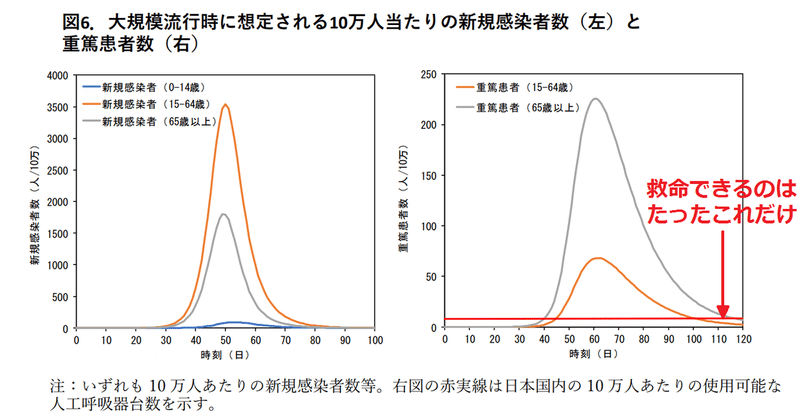
*Figure 6. Anticipated number of new infections per 100,000 in the event of a pandemic (left), and the number of the patient of sereverely ill (right)
X=days, Y=number of newly infected(L), and severely ill(R)
*In the red letters say, "only we can save this number of life"
[The following is my interpretation of the chart] About per 100,000 people, about 220 elderly and 50 young are severly ill. In other words, 270 / 100,000, so in a larger scale 100,000 out of 270,000. This is not the number of severely ill people but the number of seriously ill people (people who die if not managed by ICU). At this rate, we can provide only 10,000 respirators per 100,000 people, that meas 10,000 respirators are available. And this graph shows the number of newly infected people (3.5 million / 100,000, or 3.5 million for 100 million people) and the number of seriously ill, so 250,000 is not cumulative. Perhaps my understanding may be wrong, but considering the my layman's calculation of the assumed number of 2 million people of severlly ill and the capacity of a respirator to save life; 10,000 people multipled by rounds, estimation is that almost 2 million people may be exposed to a chance of death.
According to Professor Nakazawa’s estimation, if the cluster measures fail, the worst case scenario of 150,000 deaths would come true. This does not take into account the 10 times effect and the limitations of the ventilator mentioned above.
* Postscript: It is essential to read about the movement of the world in an easy-to-understand explanation. The English version is more comprehensible. These are mitigation and suppression strategies. The latter reduces 𝑅₀ to near zero due to city blockade. Japan's “semi-containment” strategy targets 𝑅₀ <1.
(2) Strangely low Japan’s 𝑅₀
It is also necessary to keep in mind that Japan's 𝑅₀ was lower than other countries. This is very strange, but probably accurate. If Japan’s 𝑅₀ was similar to Europe and the United States, the country would have experienced the overshoot (infection explosion) like Wuhan and the current Europe and America as of February already. The trends in the number of infected, seriously ill, and dead people in Japan have kept consistently low since January.

On the other hand, there might be a dispute that it may be because the inspection is suppressed, but the inspection suppression is only effective to shift the exponential increase by a few days, and a gentle slope has continued since January, which can not be explained by testing suppression.
But if Japan is not taking any special measures, but why is it so low? (Singapore and Hong Kong are taking extremely strict measures.) This is a mystery, but you can’t google it why. Government measures, such as cluster measures, are not the cause (they must have been around since January if so). Probably because of the awareness of hygiene for the personal protection such as hand-washing and masks, lack of body contact habits such as shaking hands and hugging, and also it is because many nerds who like two dimensions characters stay at home.
Needless to say, my comments about geeks are the joke. Since it came to the eyes of many people than I thought, it is crude but I will add a note.
If 𝑅₀ was originally high (on par with other nations), the measures to bring 𝑅₀<1 by cluster measures were probably not feasible.
2. Rationale for cluster measures
As a whole, Grantz K, Metcalf CJE, Lessler J (15th Feb 2020) Dispersion vs. Control is a basic framework, and also Nishiura H et al. "Closed environments facilitate secondary transmission of coronavirus disease 2019 (COVID-19) has shown concrete measures based on it.
(1) Characteristics of propagation of COVID19-Large variance of 𝑅₀ (Grantz paper)
Grantz's paper shows that coronaviruses have a high variance in 𝑅₀, based on Wuhan data. Many infected people do not have a secondary infection, and if so, their infectivity is low, but they are not. The reason why the virus is so infectious is that only a small portion of infected people have large secondary infections (cited below).

*Upper shows the model of influenza spread
*Lower shows the model of new corona virus spread
Influenza, for instance, causes secondary infections that are close to the average in infected people, and the infections are transmitted gradually and continuously. Although COVID19 does not cause the secondary transmission in most cases, a small number of infected individuals can cause the large secondary transmission, and thus the virus is spread widely. A large secondary infection caused by a small number of infected people is called a cluster infection.

So to speak, flu has a continuous process (or similar) to transmit, but COVID is a discrete and discontinuous process. It makes difficult to handle and predict, but there is still room for prevention. Theoretically, if the cluster infection is suppressed or suppressed in some way, 𝑅₀ <1 can be achieved because the non-cluster infections are relatively small.
(2) Elucidation of the causes of cluster measures (Nishiura's paper)
Grantz's paper showed that if cluster infections were suppressed, the 𝑅₀ <1 status could be achieved, that is, the epidemic could be converged. However, if there is no specific means to suppress cluster infection, it is just a pie in the sky. In Nishiura's dissertation shows how. Professor Nakazawa calls it a "genius idea." This paper analyzes 110 cases of infection (belonging to 11 clusters) that occurred by February 26 in Japan. The chart of the citation shows the distribution of the 27 infected cases that caused secondary infection (the chart itself was reprinted on the MHLW website with an explanation).

*The number of secondary infections by a single individual, 110 domestic cases as of February 26
X=secondary infections by a single individual, Y=frequency
*Gray=infection origin in bad ventilation
*White=infection origin from other envirionment
*(middle) 80% of the infected did not cause the secondary infection
*(below middle) the infected in bad ventilation caused secondary infection
These clusters are due to the close contact in the indoor environments such as fitness gyms, riverside restaurants, hospitals and snow festival tents. And, as shown in the figure, if the source of the infection were in a closed environment, it will cause secondary infections far more than otherwise. Unless it is a closed environment (parameter in white), secondary infection hardly occurs, and at most one or two people. In a closed environment, it causes secondary infections of up to 10 people (parameter in grey). In other words, one of the prominent causes of clusters is the closed environment. In a closed environment there is a risk of 18.7 times (95% CI: 6.0, 57.9).
The only thing shown in this paper (not peer reviewed completed) is only a closed environment. If the cluster infection occurs in a closed environment, crowded trains in large cities such as Tokyo are the perfect incubators for cluster infection. An explosive infection must should been occurring by now, however, the tendency is that cluster infections do not occur on crowded trains.
(3) Three conditions of cluster infection "closed room / crowded / close contact"
From the various data (from 2/26 onwards in the above paper), the cluster response team derived the three conditions of "closed room / crowd/ close contact" based on exercises. I presume that the analysis of the elaborate mathematical model is not yet completed.
This was clarified in the 3/9 expert meeting opinion.
What is common in places where outbreaks have been confirmed so far are: ① It was a closed space with poor ventilation,
② Many people were crowded,
③ Conversations and utterances were made at short distances (reachable when reaching each other)
The infection cluster happened in a place where the three conditions overlap at the same time. It is considered that many people were infected in these places.

Closed, crowded, close contact
Closed space, crowded place, close scene
A closed space with poor ventilation, a crowded place where many people gather, a close scene where conversation occurs within close up
*the area 3 circle overlaps has the highest risk to cause the cluster infection
These three conditions explain that cluster infection has not occurred on crowded trains (infection itself would have occurred). A crowded train satisfies the requirements of closed and crowded, but people do not talk face to face. They do not meet close contanct requirements. This is a very counter-intuitive and strange property, but it is true.
For example, in a crowded train, there are ① and ②, but ③ is not done much. However, in some cases, ③ may overlap. (View of the expert meeting on March 9)
* Postscript: There was an introduction of micro droplet infection at NHK Special. According to this, micro-drops are likely to drift even on crowded trains, and it may be more likely that airtightness will be canceled by ventilation at each station.
If all citizens can adhere to avoiding the three conditions, which is quite more simple compared to the lockdowns and city closures implemented in Wuhan and Europe and the United States, the closed environment case in the gray graph in the Nishiura paper can be expected to cut secondary infections. In other words, relatively easy behavioral changes can prevent cluster infection (not infection prevention; this difference is essential) and contain most of the corona infection.
3. Successful cluster measures
Cluster measures have two pillars.
①Early detection and early suppression of clusters that have already occurred
② Prevention and suppression of cluster generation due to behavioral changes
In the official opinion, there are three pillars:
① Early detection and early response of clusters (patient groups)
② Early diagnosis of patients, enhancement of intensive care for severely ill patients and securing of medical provision system
③Civil behavior change
However, the latter half of ② is a little different, so it is better to consider it in a different frame. In the first half, “Early Diagnosis” should also be considered from the public health perspective of detecting clusters earlier than the medical perspective of providing the best treatment. Even if a corona infection is diagnosed, only symptomatic treatment can be effective. If the sub-suppression by cluster measures is not successful and the outbreak of infection spreads, the healthcare delivery system is physically disrupted and inevitable.
What is the state of successful cluster measures?
Cluster infections rarely occur because citizens avoid the three conditions. Infections other than cluster infections (eg, workplaces, crowded trains, etc.) can occur, but they are scarce. Simple infections, excluding cluster infections, taper 𝑅₀ far below 1 and will taper off. Cluster protection is not about containment. It is containment of cluster infection. Nevertheless, the infected of the new corona virus has not been isolated in the city (it seems that there are now thousands in Japan), so the infection will occur and some mistakes will cause cluster infection may happen. Once a cluster infection has occurred, it needs to be detected early and suppressed early. If a cluster infection causes a cluster infection, it can lead to an explosive spread.
4. Cluster detection and "time diffrence of one month round trip"
(1) Role of PCR test
The main method of detecting clusters is PCR testing of severely ill persons (mainly the elderly). The corona virus is characterized by the fact that young people rarely become more severe and end up with milder and asymptomatic symptoms (the opposite occurs in older people). That is, a cluster of young people is "invisible." Young clusters are often mild and asymptomatic and have low health risks. However, there is a risk that a cluster infection may occur without realizing it, and if it is noticed, it may be too late. This is the scariest. If elderly people are involved in cluster infection, they will be severely affected and will undergo PCR tests (which are relatively common), so there will be a time lag, but eventually they will be caught by the detection network of the cluster response team. In addition, the data of the detected cluster is analyzed, and the conditions for cluster generation are identified more precisely and reliably. Detection / suppression and behavior change must be implemented as such a cycle.
(2) One month round-trip time
*This part has been added.
It is important to note the detection time lag (source of figure).

This figure is the data from Wuhan. The yellow bar on the right is the number of reported cases, and the gray bar on the left is the date of the case. Gray is what is actually happening, yellow is what the authorities know. It takes about two weeks to go though the infection, onset, worsening, testing, and reporting. The case data we see every day is two weeks old. In Wuhan, the number of cases began to grow exponentially, causing a lockdown (city blockade), at which point the exponential growth continued for two weeks. With lockdown, the increase turns into a decrease, but the effect is noticeable after two weeks. For the next two weeks you can only watch the exponential growth already occurring being reported one after another. The current situation is the same in Europe and the United States. After seeing the explosive outbreak began, they took a serious measure such as lockdown, but for the time being they had to accept the exponential growth that had already been going on. This is a definite future.
In this way, it is very difficult and terrible to deal with an object that shows exponential behavior when you can only observe the past two weeks ago. Also, if you look at the reality two weeks ago and take some action, the effect can be observed two weeks later. Cluster measures were implemented at the end of February, and the three conditions were announced at the beginning of March. The data we are looking at at this time reflects only the reality of the first half of February. And we need to wait until around March 10 to see the effect of this timing measure. There is a "time difference of one month round trip".
That is why the cluster response team is impatient. If you make a mistake, you will know it in two weeks, and the measures will take effect two weeks later. In the meantime, the exponential explosive spread may become out of control. That is why we need to speed up the distribution of information. Tests need to be expanded to run PCR tests earlier (and preferably for those with milder illnesses), to streamline the reporting process, save time, and track contacts more quickly. However, we need human resources for that!
5. Can "invisible clusters" be detected by enhanced inspection?
Some people have been following the success of Korea and demanding that inspections be strengthened. Certainly, the inspections need to be strengthened, and governments and expert meetings have stated so clearly, but the question is how the test is used for (the purpose of the test) and the test strategy. There is a lot of debate about whether to increase or suppress testing, but it is confused. It does not make much sense to discuss in a framework of increasing / suppressing inspections without clarifying the inspection strategy. Testing strategies should be considered first.
(1) Inspection strategy options
There are three possible inspection strategies:
(a) Patient examination
Examination of quasi-patients who developed pneumonia etc. and suspected corona infection
(b) Contact inspection
Active epidemiological survey (surveillance) of individuals with a confirmed contacts and contact records
(c) Strategy for mass testing of young people
A large number of mildly and asymptomatic individuals (ie, all applicants) will be tested mainly for young people.
(a) and (b) are the current inspection strategies adopted by the Japanese government. (a) Identify corona-infected patients from patients, especially those with severe illness, and (b) follow the contact links to conduct tests to detect and suppress clusters. On the other hand, cluster detection via the occurrence of severely ill patients is a detour, and it is necessary to directly test the mild or asymptomatic people who make up the “invisible cluster”. That is (c), strategy for mass testig of youg people. It seems that the tone that we should follow South Korea is vaguely assumed by this idea.
(2) Mass testing strategy for young people does not work
However, (c) the mass juvenile testing strategy does not work. It is going to collapse. There are three reasons for this, but it is essentially a low prior probability. * Correction: (A) and (B) turned upside down. (
A) Large number of false positives reaction, increased false information, and cluster detection does not work
(B) The burden on medical or isolation facilities is high due to the occurrence of false positives
(C) There are no resources to execute the strategy. Or even if it is burdensome
If you do a specific calculation, it's easy to see why it doesn't work.
Assuming 50 million people are targeted from 100 million young people. In Japan, there are thousands of infected people in the book (892 officially reported cases). If there are 10,000 people, that is 0.01%. Of the 50 million young people, 5000 are infected. There are 100 infected people and 999,900 non-infected people to test one million people. Let's make 1 million non-infected people to make it more comprehensive. It seems that the PCR test has a sensitivity of 80% and a specificity of 99%, but let's make it both 99%. Of the 100 infected people, 99 are positive and one is negative (false negative). Of the 1 million non-infected people, 990,000 are negative and 10,000 are positive (false positives). Then, there are 100,000 positives, as a result, we do not know who the 99 infected people are in the end (positive predictive value is 1%).

Moreover, there is a problem of treatment of about 10,000 positive persons. Hospitalization is out of the question, and the cost of a dedicated isolation facility is enormous. 99% of home isolation quarantine is not effective quarantine. If an anxious positive-diagnosed patients rushes to the hospital, the hospital becomes devastating. Even if a super test with a sensitivity and specificity of 99% is assumed, it cannot be used for (A) cluster detection, and (B) puts unnecessary burden on medical institutions and isolation facilities. And (C) resources to inspect 1 million people (especially laboratory technicians) are not available. Even if it could be procured, it is useless. There is something else to do. In short, tests with low prior probability should not be conducted.
* Addition: Please refer to Prof. Nakazawa's comment on inspection. The concept of sensitivity and specificity seems to be quite difficult to understand. Also, there are some claims that the specificity is 100% due to the principle of PCR, but it is beyond my ability to pursue academic discussions on estimating specificity.
(2) Why Korea went well
However, in Korea, a large number of inspections, including drive-through inspections, have been carried out to successfully curb the trend. Why is it working? (* Postscript: Quoting a graph from the Korean CDC.

First, as a premise, in terms of (C), there was a situation in which South Korea who had experienced MARS had strengthened its inspection capabilities in advance. From now on, it is probably impossible for Japan to immediately increase its testing capabilities to the level of Korea, and even if possible, there will be considerable overkill. Next, regarding both (A) and (B), there is a special circumstance in South Korea where the prior probabilities were very high among young people in specific areas. In South Korea, mega clusters have been formed among religious groups centered on young people. The youth in the Daegu region was unusually densely infected. In the case of South Korea, more than 3,000 young people were positive, but I think that half of them were infected (even at the enormous value of 1%, About.)
* Postscript: See also Iwata's Tweet about conducting drive-through inspections in Japan.
今は無効です。日本のクラスターが場所限定で、韓国のように地域的になっていないからです。北海道はやや地域的ですが、あそこですら感染者数が少なすぎてコスト効果のバランスがとれていません。
— 岩田健太郎 Kentaro Iwata (@georgebest1969) March 15, 2020
(4) Test capacity should be increased and test strategy should not be changed
The current testing strategy of (a) testing for severely ill or (b) testing for contacts derived from it should not be changed. Increasing testing capacity, expanding the scope of testing for the severely ill, and ideally to the mild, should speed up the detection of "invisible clusters" and should be done.
6. What we do
(1) Worried about the current situation (as of March 21)
As of March 21, the "last hope" for successful semi-containment through cluster measures has emerged, but concerns about explosive spread (overshoot) still remain. I think there are two major concerns at this time; ①Is it possible to control the spread of infection in Osaka and Hyogo prefectures? ② how we reduce the social atmosphere of self-restraint
In relation to ①, the recent infectious concern was at Hokkaido. I did not follow the details, but it seems that the spread of the infection has led to loss of control following the opening of the Snow Festival. To describe more, the number of infected people increased through the festival, but they did not know who was infected from (unlinked infected people) - this is a sign that the number of invisible clusters is happening. The governor of Hokkaido declared an emergency and decided to cooperate with the cluster countermeasures team to suppress the spread of the infection (the details of the expert meeting material on March 19). This is called the Hokkaido model.
At the moment, Osaka and Hyogo prefectures seem to be in a similar situation. The cluster countermeasures team seems to be discussing countermeasures, but it seems that cooperation with the governor of Osaka and Hyogo Prefecture has not been successful. Because even Governor Omura and the mayor Kawamura in Aichi Prefecture cooperate well, I wish them to discard their estrangement, and cooperate together.
The simultaneous closing of school was announced by Prime Minister Abe without hearing the opinions of the Expert Meeting and the Cluster Task Force. The members of the expert council criticize it very sharply, and Prof. Nakazawa also rated it as "foolish." However, there are no comments that go too far at the press conference of the expert meeting, for they can't quarrel with the government.
I thought it would make sense to change the public's consciousness to "this is a tough situation." However, on the contrary, when the decision not to extend the school shut-down was announced, it seemed that the tention of crisis had been somehow relaxed, saying that it was safe now. The weather was nice during the three-day holiday, and the crowds were considerable. A large-scale event seems to be held. With the relaxation of the self-restraint mood, new clusters may appear one after another. The three conditions seem to be fairly widespread, but lack of experience and data on how strictly we need to manage this principles.
(3) Two-way risk communication
The essence of the strategy of the Expert Meeting and the Cluster Task Force was to identify the three conditions of "closed room, dense and close contact," and to find a solution to change the behavior of citizens by thoroughly informing the three conditions. Considered this theory of cluster measures is correct (and will be verified by further data), whether or not we can fulfill the three conditions determines Japan’s future. From the perspective of the Expert Meeting and the Cluster Task Force, the key to success is the risk communication with the general public.
But risk communication in expert meetings is by no means sufficient. When announcement was made by an infection expert on February 24, “the next 1-2 weeks is the vital period whether the corona virus rapidly expands or is going to end,” I tried to convince myself if experts would say so, meanwhile, I wondered how much it makes sense to earn these times.
これから1~2週間が瀬戸際だとのこと。
— 弁護士 吉峯耕平(「カンママル」撲滅委員会) (@kyoshimine) February 24, 2020
非常事態だ。
政府専門家会議の見解全文「完全な感染防御、難しい」: 日本経済新聞 https://t.co/rkzxNo3cz7
これから1~2週間が瀬戸際だとのこと。
— 弁護士 吉峯耕平(「カンママル」撲滅委員会) (@kyoshimine) February 24, 2020
非常事態だ。
政府専門家会議の見解全文「完全な感染防御、難しい」: 日本経済新聞 https://t.co/rkzxNo3cz7
On February 24, there was a move to set up a cluster countermeasure team, which was set up on the following day. The three conditions are specified a little later, since the data up to February 26 is used and the information is available on March 2-3. A clear official announcement is March 9th. In other words, we are setting up a cluster response team, launching effective exercise, analyzing the data obtained, identifying the three conditions, and quickly making public relations activities. A miraculous sense of speed. There is no indication, but I guess that Mr. Kato of Ministry of Health, Labor and Welfare exerted his leadership and proceeded from the top down.
My first contact to the information on cluster measures was on March 12 (an interview with Dr. Imamura), and on the 13th, I watched a video of the conversation between Prof. Omi and Prof. Yamanaka (published on the 8th), and finally got an overview. On the 16th, I came to understand as I describe in this article when visited Prof. Nakazawa's website.
[tweet]
Cluster protection is a strange strategy that takes advantage of the strange nature of the new corona virus. Contrary to conventional theory and common sense, it is hard to understand. The rapidly-made cluster response team sends out the information at an incredible speed while bustering the cluster on the spot, but still, they do not afford to implement a public relations strategy necessary for public awareness. A follow-up public relations system will be in place shortly, but the speed is vital in fighting against this virus. Expert meetings and cluster response teams are fighting the virus with limited resources and under heavy pressure. The use of such phrase makes me hesitate, but the intellectuals in the field should support the fight against the virus by actively chewing information and promoting risk communication. Don't just wait for information.
At a press conference on March 19, Professor Nishiura's appearance looked painful.
If you fail, the situation will be miserable where you want to cover your eyes. The light of hope has come into the sight. The Japanese model seeks to find long-term sustainable options while maintaining minimal socio-economic functions, eliminating wasted parts, and saving most affected vulnerable groups. We believe there is an optimal solution, but it may not be easy for the people to make concessions. We need a process that everyone agrees on. (It is a kind of interpretation, not a transcript.)
At some point (or now?), The people may have to make serious decisions. It seems that there were many crowds during the three-day holiday and some high-risk behaviors were seen. Unless the situation in Osaka and Hyogo is improved, even a full lockdown of the Kansai area will be necessary. The explosive spread of Western infections seems to have determined that this struggle will be a long battle. Without the public understanding, we cannot win over the cluster infection. What are the limitations and what are the prospects after endurance? What awaits if you don't endure? Simply concluding a hand wash and avoiding the three conditions are the solutions may not move you forward.
If you have read all of this long note and can understand the annoying story of false positives and 𝑅R₀, you definitely understand coronavirus and cluster measures better than the public average. May be able to play the role of "spreading the cluster of knowledge". You don’t have to agree on my opinion. We need to do what we can to improve the understanding of the whole nation. Engineers contribute through open source projects. Although amateurs without knowledge of medical care and infectious disease control may remain uncertain what to dos,
The coronavirus discussions, I often felt, are heavily influenced by political position. When Professor Iwata boarded the Diamond Princess and revealed the situation, there were many people who treated him as a hero without knowing the circumstances well, and others decided that he was an intruder who messed up the site and ruined risk communication. The way you perceive it can depend on your political position. Avoiding outbreaks is a common interest in all political positions. If an explosive spread occurs, the whole of Japan will sink together, causing huge deaths. In this case, you need to calmly look at the facts, without political disputes.
(3) As an ordinary citizen: Let's run the economy while keeping the three conditions
The fight against the coronavirus is likely to take a little longer. You can tell from the news that the United States and Europe are having a lot of troubles. It is almost a war situation now. There are two things an ordinary citizen can do. (1) Protect yourself by washing your hands and gargle, and (2) Do not take high-risk actions such as involving with "closed room, crowded, close contact" so as not to infect people, but to run the economy within that range, and finally take a good balance of two.
Explosive outbreaks have occurred in Europe and the United States, but Japan has not become so serious. Some say they haven't been tested, but if more and more people are hospitalized and dying, they can't hide it. Apparently, the Japanese are seriously washing their hands and gargling. Let's continue to wash and gargle as usual.
The other mindset is to keep people from getting infected. This is important, especially if you are young. There are many young people who are infected with the corona virus and are active without any symptoms. In fact, you may be so. Everyone has to think that we may as well be infected and be careful not to infect others. In China, Europe, and the United States, lockdowns (city blockades) mean that stores are closed and citizens are taking very strict measures, such as being prohibited from going out. In Japan, excellent scholars have analyzed the data and found that avoiding the three conditions of "closed room, crowded, close contact" can prevent the spread of coronavirus.
Closed, crowded, close contact
Closed space, crowded place, close scene
A closed space with poor ventilation, a crowded place where many people gather, a close scene where conversation occurs close up
If all events and drinking parties are in the range of self-restraining and banned, it will be distress and many people will have trouble living, but if only three conditions are fulfilled, it is not so difficult to protect and the economy can be saved. If we can avoid city blockades and explosive spread, we are all happy. However, since the data is not perfect, let's cooperate carefully for a while. Even if it is tightly closed or dense, but not close contact (for example, if you wear a mask), the theory should be fine, but you may feel a bit uneasy. If possible, ventilate or reduce the density of people and avoid all three. In some industries such as entertainment and bars, the burden is heavy, but if we work together well, we may be able to find a way out while avoiding the risk of cluster infection.
Reference
I mainly relied on the following three points for understanding cluster measures.
①Publication materials of the expert meeting
②Press conference, interview video with Professor Yamanaka
③Website of Prof. Nakazawa (Kobe University)
I think that the press conference and interview video of ② is a must-see in the current situation where it is thought that risk communication has not been thoroughly implemented due to resource constraints.
* This conversation with Prof. Yamanaka is easy to understand, so you may want to look at it first.
(3) Professor Nakazawa's web is very useful and essential for understanding the current situation.
The ones written in chronological order are posted as they are, and they are cluttered, but for the time being I have sniped out the places that should be referenced (although the links will disappear).
In addition, Sean KY's NOTE, which is not an expert, seems to be useful as commentary for the general public.
The opening image was cut from a 3/2 press conference.
この記事が気に入ったらサポートをしてみませんか?