
体内から消えない人工mRNAとスパイクタンパク:ロバート・マローン博士が指摘する人工mRNAワクチンの潜在的危険性と医療公共政策の悪夢…について

ロバート・マローン医学博士が、最近の研究論文や記事を引用しながら、人工mRNAの潜在的危険性について述べたサブストックのブログ記事が興味深かったので、こちらに翻訳&解説(訳註)してみました。本文記事は↓
まず、有名科学誌「CELL」の論文のハイライトされている内容を紹介しています。(*訳註:マローン博士は、特に3)と4)に注目している)
1)ワクチン接種により、SARS-CoV-2感染よりも変異型RBD(受容体結合領域)に対するIgG抗体結合の幅が広がる
2)(ワクチンによる)最初の抗原曝露による刷り込みが、(実際の)ウイルス変異体に(暴露された時に)対するIgG抗体応答を変化させる。
3)mRNAワクチン接種者のリンパ節(= lymph node, LN )の組織検体の特徴として、胚中心*(= germinal center, GC )が豊富に生成されている。
4)ワクチンスパイク抗原とmRNAは、リンパ節の胚中心で数週間も存在し続けることが判明。(*訳註:当初の予想とは違い、通常のmRNAの様に数時間で消えないし、それによって生成されたスパイクタンパクも、1週間くらいで消えるはずが消えていない…ということ)
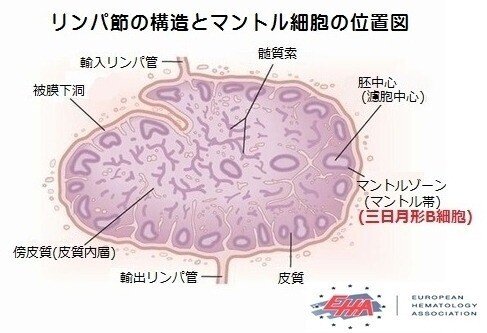
*訳註:胚中心*(= germinal center, GC )とは、免疫機能に関わる白血球(T細胞とかB細胞など)が集まる二次リンパ器官(リンパ節(= lymph node, LN )、回腸のパイエル板、脾臓)の中にある「B細胞領域(濾胞)」の内部に抗原にさらされた時に一時的にできる微小構造で、抗体を産生するB細胞が分化する場所。下がその図解↓
マローン博士のコメント→ この研究は、 mRNAとそれから生成されたスパイクタンパク質が、ヒト患者のリンパ節胚中心*内に、数週間も存在し続けることを証明するものである。私は、何十年にもわたってmRNAを扱ってきた経験から、これは通常(の自然界にあるmRNAでは)まず有り得ない事だと断言できる。
(これを可能にできる)1つの現実的な仮説は、(体内で細胞外にあるmRNAを異物と見なして排除するための)免疫反応を回避するために(このワクチンの人工mRNA内に使われた)ウリジンの代わりのプソイド(偽)ウリジンが、非常にうまく機能し過ぎて(この人工)mRNAが(体内の)通常のmRNAの自浄作用/分解経路を完全に回避しているというものである。そうであれば、注射部位の細胞に取り込まれなかった(人工)mRNAは、リンパ節(+ファイザーの動物での非臨床データが示唆するように全身**)に移動し、そこでタンパク質を生成し続けていることになる。ここで細胞傷害性タンパク質抗原とは、スパイク蛋白質である。スパイク蛋白質は、ワクチン投与後の少なくとも60日間は検出されている。ただし、この発現期間は60日間までしか検証されていない。(訳註:それ以降も続いているかもしれないが、それ以上のデータが取られていないということ)
それでは、スパイクタンパク質、それが何であり、またどのように使われているか、をおさらいしておこう(以下Daily Skepticより引用)
この新しい遺伝子ベースの『ワクチン』は全く新しい方法で作用しており、従来の(タンパク質ベースの)ワクチンとは似ても似つかないものである。それに加えて、製薬会社は元来競争的なのに、全社がSARS-CoV-2ウイルスの『スパイク・プロテイン』と呼ばれるものをターゲットにするという同じアプローチを取ったことも驚きであった。
この(スパイク)タンパク質は厄介なもので、時には「病原性タンパク質」とも呼ばれ、COVID-19の恐ろしい病態の多くを引き起こす原因そのものと認識されています(訳註:ウイルス全体でなくても、スパイクタンパクだけで、細胞を傷つけたり、血栓を起こしたりできることが判明してきた)。
論理的には、この厄介なスパイクタンパク質を不活性化するか、少なくとも減衰させ、減衰させたウイルスを用いてワクチンを開発することが懸命である。しかし、それは行われなかった。これらの「いわゆるワクチン」には問題のウイルス自体は全く含まれておらず、むしろ厄介なスパイク・タンパク質を体内で作らせる遺伝子配列が含まれているのである。
これによって、この厄介なタンパク質がどのくらい体内で作られるのか、また、遺伝子配列を注射した後に、どのくらい体内に留まるのかなどは、ほとんど分かっていない。さらに言えば、体内の複雑な生物学的システムを刺激してスパイクタンパク質を作らせるということだから、その体質の差によって作られるタンパク質の量が、人によって違うということだ。これは、スパイクタンパク質をコードする遺伝子が私たちの体内でスパイクを生成することで、私たちの免疫システムがスパイクに対する抗体を産生する反応を引き起こし、野生のウイルスが私たちに感染すると、抗体はそのスパイクタンパク質を認識し、それを攻撃して、ウイルスの悪影響を防ぐ…という考え方の元にデザインされているものだ。しかし、この方法は、感染を防いだり、感染を食い止めたりするのにはあまり適していないことが分かってきた。
私たちは、藁にもすがる思いで、これらの「いわゆるワクチン」が深刻な病気や死を防いでいると主張するのだろうか? この2年間、従来の治療薬でCovidの症状を治療してきたことからは何も学んでいないのだろうか?
これらのワクチンに含まれるスパイクタンパク質について分かっている(それ自体に毒性がある)ことを踏まえ、この研究ではワクチン接種後の血漿中のスパイクタンパク質濃度を定量的に測定しました。しかしこの様な研究は、ヒトを対象にした臨床試験を開始する前も含め、そのずっと前に(動物実験などで)特定されているべきことです。
こういったことが発表されず、調査もされなかったことは、ファイザー、バイオインテック、モデルナ、NIAID(アメリカ国立アレルギー・感染症研究所)、VRC(ワクチンリサーチセンター) とその全スタッフによる薬品規制においての重大な職務怠慢が行われていることを示しています。
プソイド(偽)ウリジンを含むこれらのワクチンを、それによる影響を十分に理解することなく、またFDA(アメリカ食品医薬品局)が(薬品に使われる)他の新しい化学物質やアジュバント添加物と同様に長期追跡調査を含む完全な前臨床毒性規制(研究結果)パッケージを要求しないまま使用させるということ自体が、ショッキングなことです。
さらに、これらのワクチンで使用されている特異的なナノ粒子の新しい使用法がありますが、これも日本でのファイザーのデータ**で示されているものしかないように、ほんのわずかな評価しかされていません。
(接種者の体内でのスパイク)タンパク質の発現(生成)が停止していないのは、(注入された)mRNA/プソイド(偽)ウリジン複合体に対する(それを分解して除去するための)免疫応答が起こっていないか、効果がないためです。 また、mRNA/シュードウリジン複合体は、通常のmRNAよりも半減期が長いのかもしれません。 その いずれにしても、これは(そういったことを事前にリスク回避するべきである)規制機関にとっては悪夢の様な事態です。
(この最悪な状態を)これ以上どう強く書けば伝わるのか分かりませんが…この技術は未熟なんです。 WHOはもっと伝統的な(方法で作られた)6種類のワクチンを承認しており、これらはすべて米国政府がライセンス供与できるものです。この『遺伝子ワクチン』が唯一の選択肢ではなかったのです。
注意すべきことは、これらのmRNAワクチンにプソイドウリジンを使用することは、唯一の選択肢ではないことです。(それなのに、どうしてわざわざそれを使用したのかという)仮説としてよく挙げられるのは、カリコ博士***がmRNAワクチンにプソイドウリジンを加えたのは、私が発明者であるオリジナルのmRNA(ワクチン技術の)特許の改良版を作るためであったというものです。というのも、既存の特許に改良を加えるカタチをとることで、新たな特許での商品化が可能になるからなのです。昔からある手口です。現に、CureVac社****のmRNAワクチンは製剤にプソイドウリジンを使っておらず、有意な免疫反応に必要でもなんでもないことを忘れないでください。次世代のmRNAワクチンの実験(動物モデルで行われることを望む)では、これらのワクチンをヒトに投与する前に、プソイドウリジン添加の問題に対処する必要があることは明らかである。
****カリコ博士についての訳註:の新しい特許ゆえにワクチン会社は、マローン博士に特許料を払わなくてい済んでいるのだと思われます。それ以前からも、マローン博士が属していた製薬会社もマローン博士に支払うはずだった特許料を全く支払っていません。また、このカリコ博士はその昔、マローン博士にmRNAワクチン技術について色々と教えてもらったこともあるのに、自分こそがmRNAワクチン技術の発明者だと名乗り、マローン博士に授与されるであろうノーベル賞を自分が貰える様に大学ぐるみで働きかけているような状態です。これらの詳細は、マローン博士の夫人、ジル・マローン博士が以下のリンクで記事にしています。(英語)
****CureVac社のmRNAワクチンについてのプレスリリース日本語版
論文からの引用は長いですが、とても重要なので読んでみて下さい。
「SARS-CoV-2 mRNAワクチン接種後の
LN (=リンパ節)内の GC (=胚中心)における
ワクチン由来mRNAとその血中内スパイク抗原の長期間に渡る検出」
(ファイザー社製の)ワクチン接種後のワクチン由来mRNAやスパイク抗原の生体内での分布の仕方、その量、その持続期間や、SARS-CoV-2感染後のウイルス抗原に関しての理解は不完全である。しかしながら、これを理解することが、免疫反応を理解する上での主要な決定要因になると考えられる。
(ファイザー社製の正式名称)『mRNA-1273』または『BNT162b2ワクチン』2回目接種後(の患者の)同側腋窩(=脇の下)から 7〜60 日目の間に(複数回に渡って)リンパ節からのコア針生検を採取した。この生検に対して、『コントロール』および『SARS-CoV-2ワクチンmRNA特異的RNAScopeプローブ』による 『in situ ハイブリダイゼーション(ISH)法』(=組織中のRNAまたはDNAが存在する"原位置 (in situ) "をRNA-RNA、RNA-DNA、DNA-DNA ハイブリダイゼーションにより検出する方法で、組織切片を用いて特定遺伝子を検出することができる)を行ったところ、ワクチン2回目接種後の、7、16、37日目に採取したリンパ節の胚中心に、ワクチン由来mRNAが検出できた。60日目のものも、数値は低いとはいえ、まだ有意な数値の特異シグナルが検出できた(図7A -7E)。
胚中心の外でワクチン由来mRNAの増殖巣が見られるのは、ごく稀であった。非ワクチン患者(n = 3人)とCOVID-19患者においても腋窩リンパ節コア針生検でも同様のワクチンプローブハイブリダイゼーションを行ったが、陰性であった(=ワクチン由来mRNAは検出されなかった)。
mRNA ワクチン接種患者の リンパ節におけるスパイク抗原(をターゲットに染める)の免疫組織化学的染色の色の濃さには個人差があったが、(全員に)2 回目接種後 16 日目に 胚中心 に豊富なスパイクタンパク質を示し,2 回目投与後 60 日目でもスパイク抗原が存在した。
スパイク抗原は胚中心の細胞の周囲に網目状に局在し、濾胞性樹状細胞の突起の染色と類似していた(図7B)。
COVID-19患者のリンパ節では、スパイク抗原の量は少なかったが、胚中心が陽性に染色されることは稀であった(図7F)。
COVID-19患者の気管支周囲にあるリンパ節の二次および一次濾胞におけるN(ヌクレオカプシド)抗原に対する免疫組織化学染色(図7F〜図7I)では、7人中5人が陽性、ヌクレオカプシド陽性濾胞の平均割合は25%以上であった。
考察:SARS-CoV-2パンデミックの世界的な災難の中での好ましい進展の1つは、様々なワクチンの迅速な設計、製造および配備であ理、その中にはウイルススパイクをコードする著しく有効なmRNAワクチン(Badenら、2021;Polackら、2020)が含まれる。
我々は、BNT162b2ワクチン接種が、重症のCOVID-19患者と同程度の濃度でスパイクおよびRBDに対するIgG免疫応答を生じさせ、同様の時間経過をたどることを見出した。
自然感染によって引き起こされる強固だが短時間で消滅するIgMとIgA免疫応答とは異なり、ワクチン接種では、初期の時点でもIgG抗体生成の顕著なバイアスを示している。
もう一度読んでみてください。スパイクのタンパク質生産量は、重症のCOVID-19患者よりも高いのです
また、この論文では、抗体反応はIgAでもIgMでもなく、IgGであることも指摘されている。IgAやIgM抗体は、IgGとは異なり、呼吸器疾患に必要な強い粘膜免疫応答を産生する(のに大切な)んです。
今回のSubstackの記事では、科学と政府・製薬企業側の不正の両面から、この論文の意味するところの表面をなぞったに過ぎない。この問題については、また今後に続きます…
論文の全文をダウンロードするには、下記のリンクをクリックしてください。
「なぜこれらのワクチンは、遺伝子技術用の
適切な安全性試験にかけられなかったのか」元製薬研究者に聞く
The Daily Skeptic 7 February 2022 by Dr. John D. Flack
「daily skeptic」のこの記事は、適切な研究が行われていないことを見事に記録しており、その理由についての質問にも答えようとしている。
私たちは、藁にもすがる思いで、これらの「いわゆるワクチン」が深刻な病気や死を防いでいると主張するのだろうか? この2年間、従来の治療薬でCovidの症状を治療してきたことからは何も学んでいないのだろうか?
おそらく、このことが大手製薬会社を、「病人を治療すること」よりも「健康な人を守る」というより収益性の高い新しいモデルを追求するように仕向けたのではないだろうか?
遺伝子ベースの「いわゆるワクチン」の時代に突入した。この新しい技術は、命が芽吹くまでの長く困難な時期と、それが何度も失敗に終わる死産を経験した。しかし、東洋から来た「未曾有の(と一応言われている)」ウイルスによって、その時が来たのかもしれない。グローバル ヘルスの緊急事態が宣言され、技術的な対応が要求され、それが待ち構えていたのである。
しかし、私たちは技術に目を奪われ、騙され、『安全で効果的な医薬品の提供』という最終目標を見失ってはいないだろうか。検査・追跡ー騒動を煽られる中で、PCR、迅速抗原検査技術、情報APP技術の適切な利用をしているだろうか?遺伝子(治療)技術は、これまで未検証であったこの技術の短期的・長期的安全性の潜在的問題を十分に検討することなく、世界規模の大量予防接種プログラムに使用する準備ができていたのだろうか?
私の目には、『テクノクラシー』(=技術主義者)が、何十年、何百年にもわたって確立されてきた基礎医学、免疫学、ウイルス学、薬学、そして公衆衛生全般の健全な原則を、踏み壊したように見える。そしてその過程で、政治的民主主義、個人の自由、言論の自由、選択の自由は危険なまでに脇に追いやられ、検閲さえされてしまったのだ。
------以下は、マローン博士のサブストックの原文の転載-------
Highlights (per the journal)
Vaccination confers broader IgG binding of variant RBDs than SARS-CoV-2 infection
Imprinting from initial antigen exposures alters IgG responses to viral variants
Histology of mRNA vaccinee lymph nodes shows abundant germinal centers
Vaccine spike antigen and mRNA persist for weeks in lymph node germinal centers
This study asserts that the mRNA and the spike protein produced persists for weeks in lymph node germinal centers in human patients. Having worked with mRNA for decades, I can attest that this is highly unusual.
One very real hypothesis is that the substitution of pseudouridine for uridine to avoid the immune response is working so well that the mRNA is completely evading the normal clearance/degradation pathways. Hence, mRNA that is not being incorporated into cells at the injection site, is migrating to the lymph nodes (and throughout the body as the non-clinical Pfizer data suggest?) and continuing to express protein there. In this case, the cytotoxic protein antigen is spike. Spike protein can be detected for at least 60 days after administration of dose. Note that the duration of the protein expression was only tested for 60 days.
The spike protein, let’s review what it is and how it is being used (from the Daily Skeptic):
These new gene-based ‘vaccines’ are working in a completely novel way – nothing remotely resembling that of traditional vaccines. Given that pharmaceutical companies work competitively it was also somewhat of a surprise they took the same approach of targeting what has been termed the ‘spike protein’ of the SARS-CoV-2 virus.
This (spike) protein is nasty – sometimes being referred to as a ‘pathogenic protein’ – and is recognised as causing many of the awful pathologies associated with the disease of COVID-19. Logically you would inactivate or at least attenuate this nasty spike protein and develop a vaccine around the attenuated virus. But that’s not what was done. These ‘vaccines’ do not contain any of the offending virus at all but rather the gene sequence that causes the nasty spike protein to be made in the body. We have little idea how much of this nasty protein is produced or for how long it lasts after an injection of the gene sequence. Furthermore, stimulating the body’s own complex biological systems to produce the spike protein will mean that the amount of protein produced will vary from person to person. The idea is that the spike protein produced by the gene encoding it elicits a response by our immune system to produce antibodies directed against the spike. When the wild virus comes along and infects us the antibodies recognise the spike protein and attack it thus preventing its nasty effects. And it does, though as we have since learnt this approach isn’t very good at preventing infection or stopping its transmission. Are we perhaps clutching at straws too in claiming that these ‘vaccines’ are preventing serious disease and death? Have we not learnt anything over the past two years in treating Covid symptoms with conventional therapeutic drugs?
Knowing what we know about the spike protein in these vaccines, the study quantitatively measured spike protein levels in plasma after vaccination. This should have been characterized long ago, including prior to beginning human clinical trials.
That this has not been published or investigated more demonstrates the gross regulatory dereliction of duty by Pfizer, Biointech, Moderna, NIAID VRC and that whole crew. Using these vaccines, which include pseudouridine without fully understanding the implications and without the FDA requiring a complete pre-clinical toxicology regulatory package, including long-term follow-up, as is done with any other unique chemical or adjuvant additive is shocking. Then there is the novel use of the unique nano particles being used in these vaccines, which also were only marginally assessed, as shown by the Japanese Pfizer data.
Protein expression is not being turned off, because the immune response against the mRNA/pseudouridine complex is either not happening or is ineffective. It may also be that the mRNA/pseudouridine complex has a longer half-life than normal mRNA. The In either case, this is regulatory nightmare.
I do not know how to write this more strongly. This technology is immature. The WHO has approved six, more traditional vaccines, all of which the US government could license. These genetic vaccines are not the only option.
To note: The use of pseudouridine in these mRNA vaccines is not the only option. It has often been hypothesized that the reason Dr. Kariko added pseudouridine to the mRNA vaccine was to make an improvement to the original mRNA patents that I was an inventor on. An improvement to an existing patent allows commercialization of that patent. It is an old trick. Remember, that Curevac does not use pseudouridine in its formulation and it is not required or necessary for a significant immune response. In the next generation of mRNA vaccine experiments (hopefully done in an animal model), it is clear that the issues of adding pseudouridine need to be addressed prior to any more of these vaccines going into humans.
I know the following from the paper is long, but it is very important.
Prolonged detection of vaccine mRNA in LN GCs, and spike antigen in LN GCs and blood following SARS-CoV-2 mRNA vaccination
The biodistribution, quantity and persistence of vaccine mRNA and spike antigen after vaccination (with the Pfizer vaccine), and viral antigens after SARS-CoV-2 infection, are incompletely understood but are likely to be major determinants of immune responses. We performed in situ hybridization with control and SARS-CoV-2 vaccine mRNA-specific RNAScope probes in the core needle biopsies of the ipsilateral axillary LNs that were collected 7-60 days after 2nd dose of mRNA-1273 or BNT162b2 vaccination, and detected vaccine mRNA collected in the GCs of LNs on day 7, 16, and 37 post vaccination, with lower but still appreciable specific signal at day 60 (Figures 7A -7E). Only rare foci of vaccine mRNA were seen outside of GCs. Axillary LN core needle biopsie of non-vaccinees (n = 3) and COVID-19 patient specimens were negative for vaccine probe hybridization. Immunohistochemical staining for spike antigen in mRNA vaccinated patient LNs varied between individuals, but showed abundant spike protein in GCs 16 days post-2nd dose, with spike antigen still present as late as 60 days post-2nd dose. Spike antigen localized in a reticular pattern around the GC cells, similar to staining for follicular dendritic cell processes (Figure 7B). COVID-19 patient LNs showed lower quantities of spike antigen, but a rare GC had positive staining (Figure 7F). Immunohistochemical staining for N antigen in peribronchial LN secondary and primary follicles of COVID-19 patients (Figures 7F - 7I) was positive in 5 of the 7 patients, with a mean percentage of nucleocapsid-positive follicles of more than 25%.
Discussion One of the positive developments amid the global calamity of the SARS-CoV-2 pandemic has been the rapid design, production and deployment of a variety of vaccines, including remarkably effective mRNA vaccines encoding the viral spike (Baden et al., 2021; Polack et al., 2020). We find that BNT162b2 vaccination produces IgG responses to spike and RBD at concentrations as high as those of severely ill COVID-19 patients and follows a similar time course. Unlike infection, which stimulates robust but short-lived IgM and IgA responses, vaccination shows a pronounced bias for IgG production even at early time point
Read that again: Protein production of spike is higher than those of severely ill COVID-19 patients!
The paper also notes that the antibody response is IgG, not IgA or IgM. IgA and IgM antibodies produce a strong mucosal immune response needed for respiratory diseases, unlike IgG.
This Substack article has only skimmed the surface of the implications of this paper in terms of both the science and the malfeasance on the part of our government and pharmaceutical corporations. There is more to come on this issue.
To get to the full paper to download, click here.
Why Weren’t These Vaccines Put Through the Proper Safety Trials For Gene Technology, Asks a Former Pharmaceutical Research Scientist The Daily Skeptic 7 February 2022 by Dr. John D. Flack
This article by the daily skeptic does a great job at documenting that appropriate studies have not been done and even attempts to answer the question why:
Are we perhaps clutching at straws too in claiming that these ‘vaccines’ are preventing serious disease and death? Have we not learnt anything over the past two years in treating Covid symptoms with conventional therapeutic drugs?
Perhaps this has driven Big Pharma to pursue a new more profitable model based on protecting the healthy rather than treating the sick? Enter the era of the gene-based ‘vaccines’. The new technologies have had a long and difficult gestation period with several stillbirths. But perhaps their time had come with the ‘unprecedented’ virus from the East. A declared worldwide health emergency demanded a technological response, and it was there in waiting. But have we been blinded and duped by technology and lost sight of the end game of providing safe and effective medicines? Was it a judicious use of the PCR, rapid antigen test technology and information APP technology to drive the test and trace fiasco?
Was the gene technology ready to be used in a mass world-wide vaccination programme without a thorough examination of the potential problems of short- and long-term safety of this previously untested technology?
In my view, technocracy has trumped the sound principles, established over decades and centuries, of basic medical practice, immunology, virology, pharmaceutical sciences and public health generally. In the process, political democracy, personal freedoms, free speech and choice have been dangerously sidelined and even censored.
この記事が気に入ったらサポートをしてみませんか?