ESICM guidelinesの「no recommendation」と「against 」は、どのような基準なのか?

ESICM guidelinesの問題点を、ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies より考察しました。特に、「no recommendation」が、どのようにして選ばれているかをポイントとしています。
Domain 3の推奨
まず、「Domain 3: High-flow nasal oxygen」の推奨を確認します。
Question 3.1: In non-mechanically ventilated patients with acute hypoxemic respiratory failure not due to cardiogenic pulmonary edema or acute exacerbation of chronic obstructive pulmonary disease (COPD), does HFNO compared to conventional oxygen therapy (COT) reduce mortality or intubation?
Recommendation 3.1
We recommend that non-mechanically ventilated patients with AHRF not due to cardiogenic pulmonary edema or acute exacerbation of COPD receive HFNO as compared to conventional oxygen therapy to reduce the risk of intubation
Strong recommendation; moderate level of evidence in favor
We are unable to make a recommendation for or against the use of HFNO over conventional oxygen therapy to reduce mortality
No recommendation; high level of evidence of no effect
次に付録を確認。付録のHFNO vs. O2のTable 4. GRADE quality of evidence rating reported for the two outcomes.の表と付録のFig2と3。



解説
Recommendation 3.1は2つの推奨から作られている(COVID-19は除外します(エビデンスがはっきり書いてないCQがあるので))。一般的なCPGでは、アウトカムを統合するが、ESICM guidelinesでは、アウトカムごと、すなわち、「reduce the risk of intubation」と「reduce mortality」を分けて推奨している。
「reduce the risk of intubation」に関しては、「Strong recommendation」であり(なぜか、死亡より、先に記載されている)、
「reduce mortality」に関しては、「No recommendation」である。
本文のSummary of the evidence(付録表・図も同じ)より、以下が推奨の根拠と考えられる。
「reduce the risk of intubation」に関しては、「解析された6つの試験における28~30日目の挿管率のプールは43%であった。メタアナリシスでは、挿管予防におけるCOTと比較したHFNOの有意な有益効果が同定された(RR 0.89、95%CI 0.81-0.97)。」より、強い推奨。
「reduce mortality」に関しては、「28日または30日死亡率の合計が20.5%であった症例では、HFNOとCOTの死亡率に統計学的に有意な差はみられなかった(相対リスク(RR)0.95、95%信頼区間(95%CI)0.82-1.09)。」より、推奨なし。
すなわち、GRADEアプローチでは、相対効果より絶対効果で判断する事が望まれているが、相対効果で行っている。また、「有意差のありなし」のみで、臨床の効果の有無を判断しており、「些細な効果・小さな効果や、最小臨床差(MID)」などは、まったく考慮されてない。そして、有意差が無い場合は、「evidence of no effect」との表現になる。これは、このCPGで一貫しているので、点推定値の効果の大きさは関係なく、有意差ありなしで判断していると思われる。(よって、GRADEダウンの「不精確さ」も評価が甘くなっている可能性があるが、そこまでは確認していない)
また、「reduce the risk of intubation」に関しては、同じ論文からのエビデンスにもかかわらず、なぜか、「reduce mortality」にはない「not due to cardiogenic pulmonary edema or acute exacerbation of COPD」の条件がついている。ともかく、同じ介入であるが、アウトカムごと推奨が異なるということで、どのように利用するのだろうか。さらには、重大なアウトカムが2つしかないというのも疑問であり、都合の悪いアウトカムを隠している疑いが懸念される(論文がなければナイと書くべき)。先にも記載したが、重大な複数のアウトカムより、その介入に対する推奨を記載すべきであり、アウトカムごとに分けるのは、利用者の混乱を招くだけである。
さらに、害・価値観・コストに関しても、考慮されていないのか、記載がないので不明である(他のDomeinには、あるので以下に記載)。そのため、「evidence of no effect」なので、「No recommendation」と自動的に決まることになる。
Domain 9では、「evidence of no effect」なのに、「We recommend against」の理由は?
ところが、
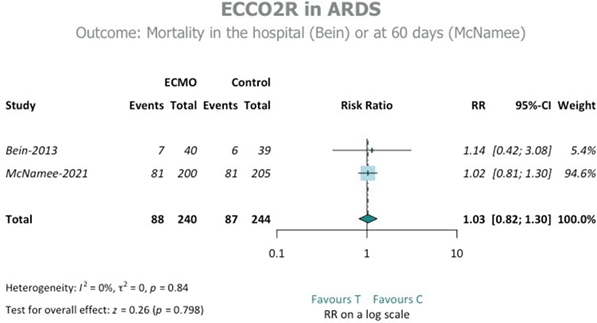
Domain 9: Extracorporeal life supportの「Question 9.2: In adult patients with ARDS, does extracorporeal carbon dioxide removal (ECCO2R) compared with conventional ventilation improve outcomes?」では、「In meta-analysis of these 2 trials, ECCO2R did not reduce mortality (RR 1.03; 95% CI, 0.82–1.3; high confidence). Patients receiving ECCO2R had fewer ventilator-free days to day 28 (mean difference − 1.21; 95% CI − 3.77 to 1.34; moderate confidence).」と、
有意差がなく「evidence of no effect」にもかかわらず、「We recommend against the use of ECCO2R for the treatment of ARDS not due to COVID-19 to prevent mortality outside of randomized controlled trials. Strong recommendation, high level of evidence of no effect.」と強い反対の推奨となっている。
付録(なぜかDomeinでなく、Group 9)に、Safetyとして、「The second trial reported a number of severe side effects attributable to the intervention [2]. Indeed, 9 patients (4.5%) suffered from a cerebral haemorrhage or from bleeding at other sites (3%) in the intervention arm, compared to none and one (0.5%), respectively, in the control arm.」との記載がある。
そして、付録のOverall quality of evidence and statistical heterogeneityの記載に、「The meta-analysis did not show any significant differences between the intervention arm and the controls in terms of mortality and ventilator-free days. Safety findings may thus justify the request for a strong recommendation not in favour of the use of ECCO2R, regardless of the level of evidence and considering that there is no evidence that the treatment could be effective. メタアナリシスでは、死亡率および人工呼吸器無使用日数の点で介入群と対照群との間に有意差は認められなかった。したがって、安全性に関する所見は、エビデンスのレベルにかかわらず、また治療が有効であるというエビデンスがないことを考慮しても、ECCO2Rの使用を支持しないことを強く推奨することを要求する正当な理由になりうる。」とある。
Figure 2.のフォレストも提示するが、たしかに、有意差がないが、付録のTable 2. Overall evidence from the meta-analysis of the two trials for the two selected outcomes(1.03を1.83と誤植あり)には、この表に、「Safety」の記載がないにも関わらず、アウトカムごとに、Againstとわざわざ記載があるという不思議な状況。
Figure 2とTable 2。

すなわち、すべてのCQで「safety outcomes」を評価して、問題がある時のみの記載なのか(害がなければナイトと記載すべきである)、介入を反対したい時のみ恣意的に「safety outcomes」を記載しているのかは、不明である。少なくとも、価値観・コストはどこにもなかったが、「害」は、一部のCQで評価しているとなる。
Domain 6(Recommendation 6)は、意味不明だが、まだ次のDomain 8よりは「害」があるだけまし
先にでてきた、「safety outcomes」は、Domein 5などにもあり、時々出現するようである。しかし、次のように、項目でなく、アウトカムの一つとして出現することがある。それが、Recommendation 6である。
Recommendation 6.3では、「害・Barotrauma」が、アウトカムの一つで、かつ、アウトカムごとの推奨でなく、まとめていたりする。ここには、「moderate level of evidence against」との記載である。この「moderate」は、Hospital mortality(有意差なし・Moderat)からで、「evidence against」は、Barotraumaのアウトカム(有意差あり・high)から作られているという、さらに混沌として意味不明(下記Table 3参照)。しかし、まだRecommendation 6.3では、「害」があるので良いが、Domain 8では、「害」もなく、有意差なしで、反対となっている(下記参照)。

Recommendation 6.4では、「Absence of evidence in favor or against the use of recruitment maneuvers, the potential safety issues led to a weak recommendation against their routine use. リクルート操作の使用に賛成か反対かのエビデンスはなく、潜在的な安全性の問題から、ルーチンの使用には弱い推奨となった。」と、何と、潜在的な安全性の問題で、「We suggest against routine use」と反対推奨となっている。
Domain 8: Neuromuscular blocking agentsでは、さらに意味不明
ドメイン8のRecommendation 8.1では、さらに不可思議な状況である。
We recommend against the routine use of continuous infusions of NMBA to reduce mortality in patients with moderate-to-severe ARDS not due to COVID-19. Strong recommendation, moderate level of evidence.
これの根拠は、本文と付録にある。付録より、表3なので、表3も見てみる。
本文:90日死亡:A meta-analysis of the two studies found an overall non-significant result, ・・・・The evaluation of overall evidence was moderate against (according to the GRADE after rating down for imprecision), and according to the risk of biases (RoB) 2 assessment tool, there was an overall low risk of bias.
28日ICU死亡:Meta-analysis identified no significant mortality reduction in the NMBA group compared to no NMBA, with a 0.80 relative risk (95% CI 0.57, 1.04), p value 0.086.
付録:90日死亡:Our evaluation of overall evidence was moderate not in favour of the intervention according to the GRADE after rating down for imprecision (Table 3).
28日ICU死亡:Thus, considering the combined effect of the five trials we downgraded evidence for inconsistency and imprecision from high to low not in support of the intervention, according to the GRADE (Table 3).

90日死亡のRRは、0.91 [0.72, 1.15]、28日ICU死亡率は、0.76 [0.56, 1.04]と、どちらも有意差がない。ということなので、「evidence of no effect」のはずだが、なぜか、上の文章のように、「against、not in favour of the intervention」となっている。よって、ドメイン3と同じ理由かと考え、「safety outcomes」の項目を探すがない。しかし、付録に、「Finally, we considered safety issues, investigating pneumothorax and critical illness neuropathy. 最後に、安全性の問題を検討し、気胸と重症神経障害を調査した。」とあり、なんと、ここでは、アウトカムの一つとなっている。しかし、「critical illness neuropathy」は、この文章に文字が出てくるだけで、他のどこにも記載がない。よって、「pneumothorax」の記載をみる。
Pneumothorax. We considered four studies investigating this outcome [1, 2, 4, 5]. The studies seemed sufficiently homogeneous to be meta-analyzed. Individual study risk of bias was rated as for mortality (low according to the RoB2, Table 2). Overal quality of evidence was rated high with the GRADE method (Table 3), and only minor concerns were found with the RoB2 tool). There was consistency across the trials and an overall clear protective effect was found in the NMBA group compared to controls (RR 0.46, 95%-CI 0.28, p 0.77, Figure 9).
Figure 9(Table 3では、0.47であるが、0.46のようだ)

NMBAのが、気胸が少ないとの結果であった(各試験に一貫性があり、NMBA群では対照群と比較して全体的に明らかな予防効果が認められた)。ということで、害がないとなる。<このnoteの著者は、腹臥位人工呼吸とNMBAの関係までは詳しくないので、どこかで抜けがあるかもしれない>
すると、ますます、「against、not in favour of the intervention」の理由が不明である。
しかし、有意差なしで、点推定値が1未満という状況にもかかわらず「evidence of no effect」とならず、推奨文に明確に、「recommend against」との記載より、このCPGでは、SRの結果も、NMBAに反対との結果だったと判断していると思われる(このnoteの著者は英語が苦手である)。
まったくもって、意味不明で困惑している。
筋弛緩薬の推奨について
他の診療ガイドラインもみてみると、ESICM 2023(2017年にはCQがなかったので新しいCQ)のみが、反対の推奨である。
ESICM 2023:Recommendation 8.1 We recommend against the routine use of continuous infusions of NMBA to reduce mortality in patients with moderate-to-severe ARDS not due to COVID-19. Strong recommendation, moderate level of evidence.
ATS 2023:Question 3: Should Patients with ARDS Receive Neuromuscular Blockade? Recommendation:We suggest using neuromuscular blockade in patients with early severe ARDS (conditional recommendation, low certainty)
JAPAN 2021:CQ31:中等症もしくは重症の成人ARDS患者の早期に筋弛緩薬を使用するべきか? 推奨:中等症または重症の成人ARDS患者において,早期に筋弛緩薬を投与することを条件付きで推奨する(条件付き推奨/非常に低い確実性のエビデンス:GRADE 2D)。
JAPAN: https://www.jsicm.org/publication/pdf/220728JSICM_ihardsg.pdf
エビデンスサマリーよりの結果は、以下の通りであり、特に、ESICMの結果が違うこともない。
ESICM 2023:ICU mortality (5 study) RR 0.80, 95% CI 0.57-1.04
ATS 2023:mortality (7 study) RR 0.74, 95% CI 0.56–0.98
JAPAN 2021: 生存(5研究)1,000人あたり84人増加, 95%信頼区間 39人減少~ 236人増加
参考#1:death at 28 days (5 study) RR 0.90, 95% CI 0.78–1.03
#1 : Ho ATN, Patolia S, Guervilly C. Neuromuscular blockade in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials. J Intensive Care. 2020 Jan 28;8:12. doi: 10.1186/s40560-020-0431-z. PMID: 32015880; PMCID: PMC6986163.
やはり、ESICMの反対の理由が不明である。丁寧に解説してある、野原先生のスライドや、よく参考にさせてもらっている、EARLの医学ノートのブログでも、理由の記載はなかった。
ネットでさらにコメントなど調べると、以下の“ESICM guidelines on acute respiratory distress syndrome 2023”- a short summaryの文章がみつかった。「中等度から重度のARDS患者に適用した場合、深い鎮静を伴う神経筋遮断薬の使用の有益性は示されていない。気胸を発症するリスクのある患者でも、神経筋遮断薬の使用は有益である。」との翻訳ですが、「有用性は示されてない。気胸リスク患者でも、有益」って文章、おかしく思うのは私だけだろうか?
2.9. Neuromuscular blocking agents
The new ESICM guidelines do not recommend the use of neuromuscular blocking agents in non-COVID-19 related moderate to severe cases of ARDS. Despite the fact that neuromuscular blockade reduces the work of breathing and patient-ventilator asynchrony, it can also result in adverse outcome due to neuromuscular weakness. This recommendation is based on the new evidence that was collected during the Reevaluation of Systemic Early Neuromuscular Blockade (ROSE) trial which as compared to the previous ARDS et Curarisation Systematique (ACURYS) trial, do not show any benefit of the use of neuromuscular blocking agents with deep sedation when applied to moderate-to-severe ARDS patients. Those patients who are at risk of developing pneumothorax may still get benefit from the use of neuromuscular blocking agents.
DeepL翻訳:ESICMの新ガイドラインでは、COVID-19に関連しない中等度から重度のARDS症例では、神経筋遮断薬の使用を推奨していない。神経筋遮断は呼吸の仕事と患者と人工呼吸器の非同期性を減少させるという事実にもかかわらず、神経筋力低下による有害な転帰をもたらす可能性もある。この推奨は、Reevaluation of Systemic Early Neuromuscular Blockade (ROSE)試験で収集された新しいエビデンスに基づくもので、以前のARDS et Curarisation Systematique (ACURYS)試験と比較すると、中等度から重度のARDS患者に適用した場合、深い鎮静を伴う神経筋遮断薬の使用の有益性は示されていない。気胸を発症するリスクのある患者でも、神経筋遮断薬の使用は有益である。
次に、Muscle relaxants in ARDS – The final verdict with the updated evidenceという論文があった。ここでは、ESICMとATSの推奨が逆とはあるが、なぜ、ESICMが反対かの理由は言及されてなかった。
The ventilatory strategies in moderate-to-severe acute respiratory distress syndrome (ARDS) with PaO2:FiO2 150 or lower (arterial partial pressure of oxygen: fraction of inspired oxygen) are an area of active research. The European Society of Intensive Care Medicine (ESICM) and the American Thoracic Society (ATS) published their updated guidelines for ARDS in 2023.[1,2] The updated recommendations regarding the use of neuromuscular blocking agents (NMBAs) are interestingly opposite to each other. The ESICM recommended against the use of a continuous infusion of NMBA.[1] Meanwhile, the ATS suggested in favour of using infusion or boluses of NMBAs.[2] On the surface, these are seemingly contradictory statements. Since the evidence block cited in both documents is similar, it is critical to review said evidence to understand the reason behind the recommendations and position of NMBAs in the current management strategy.
結局、「ACURASYS試験では予防効果が報告されたが、最新のROSE試験では有意ではない結果が示された」ので、「だったら、NMBAsは使わなくていいんじゃねぇ~」というノリだったのではないか、というのが、私の推測です。
まとめ
アウトカムをまとめて推奨していない(アウトカムごとに推奨が基本だが、「害」のアウトカムは、死亡のアウトカムとまとめている時もあり一貫性がない)
重大なアウトカムをすべて評価したか不明(明らかに少ない)
有意差がなければ、evidence of no effectと判断している
有意差と「害」がなければ(害は隠してあるのかは記載がないので不明)、「no recommendation」と自動的に判断されている
「害」の評価が、一部のCQにしか記載がなく、別項目になったり、アウトカムに含まれたり一貫性がない
「害」は、エビデンスがなくても、潜在的な懸念だけでも、反対の根拠となる
「価値観」「コスト」の評価はされてない
この記事が気に入ったらサポートをしてみませんか?