43章 病歴と身体診察

History and Physical Examination of the Musculoskeletal System
キーポイント
筋骨格系疾患の主な症状は、疼痛、関節のこわばり、腫脹、運動制限、脱力、疲労、機能低下などである。
筋骨格系疾患の適切な理学診断には、解剖学的構造、運動面、特に滑膜の構造を理解することが不可欠である。
はじめに
正しい診断を下すためには、筋骨格の症状が極めて重要である。問診では、患者が何を意味して症状を述べているのかを正確に理解することが含まれなければならない。医師は、症状の発現、部位、進行パターン、重症度、増悪因子、緩和因子、関連症状について詳しく説明しなければならない。交感神経症状と心理社会的ストレッサーとの関係も重要であり、これを明らかにする必要がある。症状が患者の機能のあらゆる側面に与える影響を評価し、治療の指針とする。
現在行っている治療や以前に行った治療が、 疾患の経過にどのような影響を及ぼしているかは、現在の症状を理解する上で有用である。抗炎症薬やグルココルチコイド系薬剤に対する反応は、炎症性疾患を示唆している。しかし、このような反応は炎症性リウマチ性疾患に特有なものではないので、病歴と身体所見を総合的に考慮する必要がある。推奨された治療法への不遵守は、患者が改善しないことの説明として、治療の失敗と区別されなければならない。
医師が患者の病歴を聴取している間、患者は病気の性質とそれに対する反応について言語的・非言語的な手がかりを提供する。初期の関節リウマチ(RA)の患者は、関節内圧や痛みを最小限にするために、手を曲げた姿勢をとることがある。患者によっては過度に心配することもあるが、症状に対して不適切なほど無関心に見えることもある。効果的な治療を開始するためには、医師は患者の病気に対する理解と態度を理解しなければならない。
Pearl: 朝のこわばりは炎症性関節症に特異的なものではなく、線維筋痛症、パーキンソン病などの神経障害、睡眠関連呼吸障害の患者にもみられることがある。
Comment: Morning stiffness is not specific for inflammatory arthropathies and may be described by patients with fibromyalgia or chronic idiopathic pain syndromes, neurologic disorders such as Parkinson’s disease (although generally without limbering up), and sleep-related breathing disorders.
こわばりの持続時間が違いますね。朝のこわばりが 1 時間以上続く場合は、活動性の炎症性関節炎以外ではめったに起こりません。朝のこわばり、または長期間運動をしなかった後のこわばり(「ゲル化現象」)は、すべての炎症性関節症で見られます. (J Rheumatol. 1999 May;26(5):1015-7.)
Pearl: 肥満患者の関節腫脹は、真の滑膜炎を反映していない場合もあり、疾患活動性の過大評価につながる可能性がある。
Comment: Diffuse soft tissue swelling can occur because of venous or lymphatic obstruction, soft tissue injury, or obesity. The description of swelling in patients with such conditions usually is ill defined or is not in a distribution of particular joints, bursae, or tendons. Obese patients may interpret normal adipose tissue over the medial aspect of the elbow, the knee, or the lateral aspect of the ankle as joint swelling.
びまん性の軟部組織腫脹は、静脈やリンパ管の閉塞、軟部組織損傷、肥満が原因で起こりうる。肥満の患者では、肘内側、膝、足首の外側の脂肪組織を関節の腫脹と間違えることがある。
・こういう場合こそ関節エコーの活躍の場ですね。(BMC Musculoskelet Disord. 2017; 18: 99.)
Pearl: 筋力低下の時間的経過は、診断に重要である。
Comment: Weakness of sudden onset without trauma often indicates a neurologic disorder, such as an acute cerebrovascular event, which generally results in a fixed, nonprogressive deficit. Weakness of insidious onset more often suggests a muscle disease, such as an inflammatory myopathy (e.g., polymyositis). The latter tends to be ongoing and progressive. Weakness that is intermittent suggests a disorder of the neuromuscular junction, such as myasthenia gravis. Patients with this disease may describe muscle fatigue with activity as opposed to true weakness.
突然の脱力は、急性脳血管障害のような神経学的障害が多く、固定的で非進行性の欠損が生じる。慢性の筋力低下は、炎症性ミオパチー(例:多発筋炎)のような筋疾患が多く、進行性で継続的である。間欠的な筋力低下は、重症筋無力症などの神経筋接合部の障害を示唆する。これらの患者は、真の筋力低下とは異なり、活動時に筋疲労を訴えることがある。
重症筋無力症(MG)は活動時の筋疲労なんですね、not 筋力低下。「変動のある筋力低下」をみたらAchR抗体(MGの9割で陽性)をオーダーしても良いでしょう。
MGと自己免疫疾患合併例多いです。(Rheumatology (Oxford) . 2019 Jan 1;58(1):135-143.)
Pearl: クレピタス(crepitus)は、運動によって生じる耳障りな、または耳障りな感覚のことである。正常な関節でも聴取されることがある。
comment: Crepitus is a palpable or audible grating or crunching sensation produced by motion.
関節内からのクレピタスは、運動中に靭帯や腱が骨表面上で滑ることによって生じる亀裂音や破裂音で通常、関節疾患の診断にはあまり寄与せず、正常な関節でも聴取されることがある。
Pearl: ROMも評価する。
Comment: The S-T-L system has been used historically to record the degree of swelling (S), tenderness (T), and limitation of motion (L) of each joint on the basis of a quantitative estimate of gradation.
S-T-Lシステムは、各関節の腫脹(S)、圧痛(T)、可動域制限(L)の程度をグラデーションの定量的推定値に基づいて記録するために歴史的に使用されてきた。例えば、「第2中手指節関節と第3中手指節関節に2+の腫脹がある」というように、関節所見を物語形式で記述する方が簡単である。グレード0は腫脹なし、グレード1は触知可能な滑膜肥厚、グレード2は正常な関節輪郭の消失、グレード3はMCP関節の率直な嚢胞性腫脹を示す。
指と手掌の距離の定量化の方法もある:指尖手掌距離(tip palm distance);TPD

Pearl: 顎関節痛は、炎症性関節炎を伴わない患者に発症することがあり、顎関節症と一致する。この症候群は、歯軋りに起因すると考える研究者もおり、線維筋痛症に似た筋膜性疼痛の一種である可能性が高い.
Comment: Arthralgias of the temporomandibular joint may develop in patients without inflammatory arthritis, consistent with temporomandibular joint syndrome.
Pearl: 胸鎖関節の圧痛は、実際の腫脹よりもはるかに頻度が高い。
腫脹を伴わないこれらの関節の圧痛は、肋軟骨炎(costochondritis)と呼ばれている。実際の腫脹がある場合は、Tietze症候群(Tietze syndrome)と呼ばれることがある。
Comment: Tenderness of these joints without actual swelling has been termed costochondritis; if actual swelling is present, Tietze’s syndrome may be the term used.
胸鎖関節炎単独では化膿性/IEが気になります。
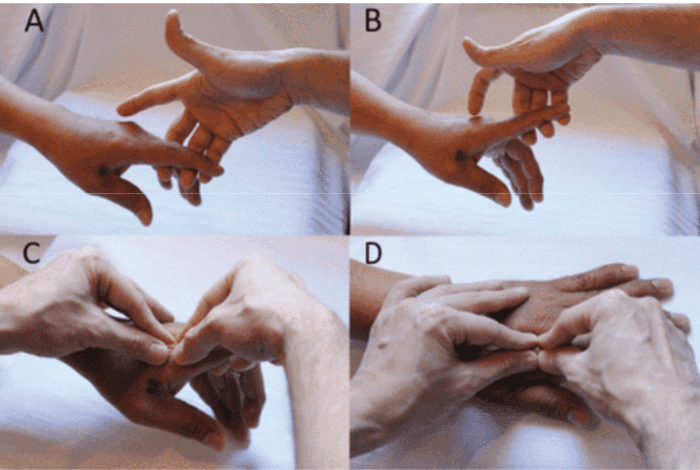
Pearl: 背側4本指法は、歴史的な2本指法に比べて臨床的滑膜炎に対する感度と陰性的中率が高く、超音波所見との相関も高い。
(A)検査者の利き手の第3~5指を約45度伸展させて指を支える。
(B)両手の親指と人差し指で中手指節関節の背側表面を遠位関節線と近位滑膜凹部の両方で触診し、「ひし形」を形成する。検査者は滑膜の肥厚と滲出液をballottementで指摘する。
Comment: The dorsal four-finger technique may have greater sensitivity and negative predictive value for clinical synovitis as compared to the historical two-finger technique and correlates better to ultrasonographic findings.20 It is especially helpful in examining the small joints to compare one with another to detect subtle synovitis.
J Rheumatol . 2018 Mar;45(3):329-334.
こんな触診法があるんですね。
Pearl: 膝窩嚢胞の急性破裂および解離は、疼痛、熱感、発赤、腫脹を伴うことから血栓性静脈炎を模倣することがある。
Comment: Acute rupture and dissection of a popliteal cyst can mimic thrombophlebitis.
膝窩嚢胞が破裂し、ふくらはぎの筋肉に剥離することがあり、肥大し、充実感を触知することができる。嚢胞が二次的な静脈閉塞やリンパ管閉塞を引き起こしている場合、浮腫がみられることがある。おそらく、深部静脈血栓症よりも RA患者の片側ふくらはぎの腫脹の原因として一般的だろう。
まずエコーでDVTを除外します。膝窩の出血班(BMC Musculoskelet Disord. 2018 Sep 24;19(1):345.)、内踝の三日月徴候(J Gen Fam Med. 2019 May 17;20(5):215-216.)が診断の役に立ちます。
Pearl: 足関節の筋力の一般的な評価は、患者につま先歩きと踵歩きをさせることで得ることができる。
つま先歩きと踵歩きが十分にできれば、足関節の屈筋と伸筋の筋力は正常と判断できる。これができない場合は、個別に筋力を検査することが望ましい
Comment: A general assessment of muscular strength of the ankle can be obtained by asking the patient to walk on toes and on heels. If the patient can walk satisfactorily on the toes and on the heels, the muscle strength of the flexors and extensors of the ankle can be considered normal. If this cannot be accomplished, it is desirable to test the muscles individually.
つま先歩きは屈筋、踵歩きは伸筋を使います。
この記事が気に入ったらサポートをしてみませんか?