イベルメクチンの予防的利用(インド)についての論文

2020年9月-10月にかけて行われた研究です。対象はCOVID-19患者を重点的にみているAIIMSの医療従事者のみで、3532人(うち、非投与者1147人)が参加しています。
盲検・ランダム化試験ではないことに注意です。
元→https://assets.researchsquare.com/files/rs-208785/v1/d6ff79a3-d354-4aba-a6b0-4bc123bbd225.pdf
・・・・・・・・・・・・・・・
Prophylactic role of ivermectin in SARS-CoV-2 infection among healthcare workers
医療従事者のSARS-CoV-2感染におけるイベルメクチンの予防的役割
Abstract
Background
Healthcare workers (HCWs) are vulnerable to getting infected withSARS-CoV-2.
医療従事者(HCW)は、SARS-CoV-2に感染しやすくなっています。
Preventing HCWs from getting infected is a priority to maintain healthcare services.
医療従事者が感染するのを防ぐことは、医療サービスを維持するための優先事項です。
The therapeutic and preventive role of ivermectin in COVID-19 is being investigated.
COVID-19におけるイベルメクチンの治療的および予防的役割が調査されています。
Based on promising results of in vitro studies of oral ivermectin, this study was conducted with the aim to demonstrate the prophylactic role of oral ivermectin in preventing SARS-CoV-2 infectionamong HCWs at All India Institute of Medical Sciences (AIIMS), Bhubaneswar.
経口イベルメクチンのinvitro研究の有望な結果に基づいて、この研究は、ブバネシュワールのオールインディアインスティテュートオブメディカルサイエンス(AIIMS)の医療従事者のSARS-CoV-2感染予防における経口イベルメクチンの予防的役割を実証することを目的として実施されました。
Methods
A prospective cohort study was conducted at AIIMS Bhubaneswar, which provides both COVID and Non-COVID care since March 2020.
前向きコホート研究がAIIMSブバネシュワールで実施され、2020年3月からCOVIDと非COVIDの両方のケアを提供しています。
All employees and students of the institute who provided written informed consent participated in the study.
書面によるインフォームドコンセントを提供した研究所のすべての従業員および学生が研究に参加した。
Uptake of two-doses of oral ivermectin (300 μg/kg at a gap of 72 hours) was considered as exposure.
経口イベルメクチンの2回投与(72時間のギャップで300μg/ kg)の摂取を曝露と見なしました。
The primary outcome of the study was COVID-19 infection in the following month of ivermectin consumption diagnosed by RTPCR as per Government of India testing criteria guidelines.
この研究の主な結果は、インド政府の試験基準ガイドラインに従ってRTPCRによって診断されたイベルメクチン消費の翌月のCOVID-19感染でした。
The log-binomial model was used to estimate adjusted relative risk, and the KaplanMeier failure plot was used to estimate the probability of COVID-19 infection with follow-up time.
対数二項モデルを使用して調整された相対リスクを推定し、カプランマイヤー失敗プロットを使用して、フォローアップ時間によるCOVID-19感染の確率を推定しました。
Results
Of 3892 employees, 3532 (90.8%) participated in the study.
3892人の従業員のうち、3532人(90.8%)が調査に参加しました。
The ivermectin uptake was 62.5% and 5.3% for two-doses and single-dose, respectively.
イベルメクチンの取り込みは、2回投与で62.5%、1回投与で5.3%でした。
Participants who took ivermectin prophylaxis had a lower risk of getting symptoms suggestive of SARS-CoV-2 infection(6% vs 15%).
イベルメクチン予防を行った参加者は、SARS-CoV-2感染を示唆する症状を示すリスクが低かった(6%対15%)。
HCWs who had taken two-doses of oral ivermectin have a signicantly lower risk of contracting COVID-19 disease during the following month (ARR 0.17; 95% CI, 0.12-0.23).
経口イベルメクチンを2回服用した医療従事者は、翌月にCOVID-19感染のリスクが大幅に低くなります(ARR 0.17; 95%CI、0.12-0.23)。
Females had a lower risk of contracting COVID-19 than males (ARR 0.70 95% CI, 0.52-0.93).
女性は男性よりもCOVID-19に感染するリスクが低かった(ARR 0.70 95%CI、0.52-0.93)。
The absolute risk reduction of SARS-CoV-2 infection was 9.7%.
SARS-CoV-2感染の絶対リスク低減は9.7%でした。
Only 1.8% of the participants reported adverse events, which were mild and self-limiting.
参加者の1.8%のみが、軽度で自己制限的な有害事象を報告しました。
Conclusion and relevance
Two-doses of oral ivermectin (300 μg/kg given 72 hours apart) as chemoprophylaxis among HCWs reduces the risk of COVID-19 infection by 83% in the following month.
医療従事者間の化学的予防として経口イベルメクチンを2回投与(300μg/ kgを72時間間隔で投与)すると、翌月のCOVID-19感染のリスクが83%減少します。
Safe, effective, and low-cost chemoprophylaxis have relevance in the containment of pandemic alongside vaccine.
安全で効果的かつ低コストの化学的予防法は、ワクチンと並んでパンデミックの封じ込めに関連しています。
Introduction
The COVID-19 pandemic that started as an outbreak in Wuhan, Hubei Province of China in December 2019 has affected around 50 million people and caused the death of approximately 1.2 million people in 11 months.
2019年12月に中国湖北省武漢で発生したCOVID-19のパンデミックは、約5,000万人に影響を及ぼし、11か月で約120万人が死亡しました。
In India, about 8.5 million people have suffered, and 126000 people have died due to this disease.
インドでは、約850万人が苦しんでおり、この病気のために126000人が亡くなりました。
Although healthcare workers (HCWs) represent less than 3% of the population in the large majority of countries and less than 2% in almost all low- and middle-income countries, around 14% of COVID-19 cases reported to the World Health Organization (WHO) are among HCWs, with the proportion reaching as high as 35% in some countries.
医療従事者(HCW)は、大多数の国では人口の3%未満、ほとんどすべての低中所得国では2%未満ですが、世界保健機関(WHO)に報告されたCOVID-19症例の約14%は医療従事者の中にあり、一部の国ではその割合が35%に達します。
HCWs are more vulnerable to infection due to the very nature of their occupation, and ensuring their safety is of paramount importance in a functioning health system.
医療従事者は、その職業の性質上、感染に対してより脆弱であり、機能する医療システムでは、医療従事者の安全を確保することが最も重要です。
Therefore, prevention of COVID-19 disease among HCWs is a priority for all administrators and governments.
したがって、医療従事者の間でのCOVID-19感染の予防は、すべての管理者と政府にとって優先事項です。
Despite the high advocacy on behavioural prophylaxis since the start of the pandemic, cases and deaths keep on increasing, indicating that only behavioural prophylaxis may not be enough to control the COVID19 pandemic.
パンデミックが始まって以来、行動予防に関する高い支持がありますが、症例数と死亡数は増え続けており、COVID19パンデミックを制御するには行動予防だけでは不十分である可能性があることを示しています。
In addition to behavioural prophylaxis, there is a need for an alternate safe intervention that can provide protection against COVID-19.
行動の予防に加えて、COVID-19に対する保護を提供できる代替の安全な介入が必要です。
To date, there is no effective cure or vaccine available to treat or protect people.
現在のところ、人々を治療または保護するために利用できる効果的な治療法やワクチンはありません。
The benecial role of ivermectin in the prevention, as well as treatment of COVID-19, has been explored in the recent past.
COVID-19の予防と治療におけるイベルメクチンの有益な役割は、最近調査されてきました。
The well-known in vitro study by Caly et al., observational studies, and an open-label randomized controlled trial conducted so far have suggested the potential role of ivermectin as chemoprophylaxis for prevention of COVID-19.
Calyらによるよく知られたinvitro研究・観察研究・これまでに実施された非盲検ランダム化比較試験では、COVID-19の予防のための化学的予防としてのイベルメクチンの潜在的な役割が示唆されています。
We noticed an increasing number of HCWs getting infected withSARS-CoV-2 infectionin early September 2020 at our hospital, which was negatively impacting on the healthcare services we had to provide.
2020年9月初旬に当院でSARS-CoV-2感染に感染する医療従事者の数が増加していることに気づきました。これは、提供する必要のある医療サービスに悪影響を及ぼしていました。
After carefully assessing the published information on ivermectin, we decided to investigate the role of ivermectin prophylaxis in the prevention of COVID-19 among HCWs following one month of administration in our hospital, which is a tertiary care teaching hospital in Eastern India.
イベルメクチンに関する公開情報を注意深く評価した後、インド東部の三次医療教育病院である当院で1か月間投与された後、医療従事者のCOVID-19の予防におけるイベルメクチン予防の役割を調査することにしました。
Methods
Aim
To demonstrate the prophylactic role of oral ivermectin in preventing SARS-CoV-2 infectionamong HCWs at All India Institute of Medical Sciences (AIIMS), Bhubaneswar.
ブバネシュワールのオールインディアインスティテュートオブメディカルサイエンス(AIIMS)で、医療従事者のSARS-CoV-2感染予防における経口イベルメクチンの予防的役割を実証すること。
Design
A prospective cohort study 前向きコホート研究
Study Setting
The study was conducted at the All India Institute of Medical Sciences (AIIMS), Bhubaneswar, India, during September-November 2020.
この調査は、2020年9月から11月にかけて、インドのブバネシュワールにあるオールインディアインスティテュートオブメディカルサイエンス(AIIMS)で実施されました。
Study cohort
All staff members of the institute formed the study cohort, which included the clinical staff engaged in inpatient care activities, administrative staff, and students.
研究所のすべてのスタッフは、入院治療活動に従事する臨床スタッフ、管理スタッフ、および学生を含む研究コホートを形成しました。
Written informed consent was obtained from all participants for inclusion in the study.
書面によるインフォームドコンセントは、研究に含めるためにすべての参加者から得られました。
Telephonic data collection was done from all study participants using administrative records.
電話によるデータ収集は、管理記録を使用してすべての調査参加者から行われました。
The study participants were recruited from 20/09/2020 to 30/09/2020, followed up after one month of taking oral ivermectin from 20/10/2020 to 30/10/2020 to assess the outcome.
研究参加者は2020年9月20日から2020年9月30日まで募集され、2020年10月20日から2020年10月30日まで経口イベルメクチンを1か月服用した後、結果を評価するためにフォローアップされました。
Exposure and Outcome
Based on a consensus statement prepared by experts from the various departments of the hospital, on September 17, 2020, a decision was taken to provide a prophylactic dose of oral ivermectin to HCWs and students. [Panel 1]
病院のさまざまな部門の専門家によって作成されたコンセンサスステートメントに基づいて、2020年9月17日に、医療従事者と学生に予防用量の経口イベルメクチンを提供することが決定されました。 [Panel 1]
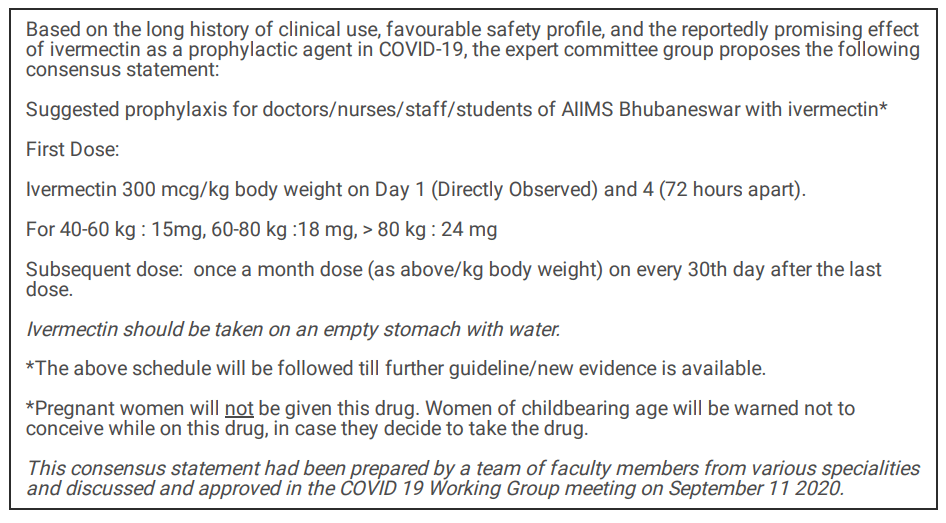
The consensus statement recommended and approved a regimen of 300 μg/kg body weight with the first two doses taken 72 hours apart, followed by a once-monthly dose on the 30th day from the last dose.
コンセンサスステートメントでは、最初の2回の投与を72時間間隔で行い、最後の投与から30日目に月に1回投与する、300μg/ kg体重のレジメンを推奨および承認しました。
Ivermectin was made available free of cost to the HCWs.
イベルメクチンは医療従事者に無料で提供されました。
Intake of two-doses of oral ivermectin (300 μg/kg at a gap of 72 hours) was considered as exposure.
経口イベルメクチンの2回投与(72時間のギャップで300μg/ kg)の摂取を曝露と見なしました。
The outcome was defined as a confirmed case of COVID-19 detected by RT-PCR.
結果は、RT-PCRによって検出されたCOVID-19の確認された症例として定義されました。
Healthcare workers were tested following the Government of India testing strategy for COVID-19 at the institute.
医療従事者は、研究所でのCOVID-19に関するインド政府のテスト戦略に従ってテストされました。
Furthermore, the HCWs were followedup through telephonic calls to conrm their COVID-19 status after a month of distribution of ivermectin prophylaxis.
さらに、医療従事者は、イベルメクチン予防の1か月の配布後、COVID-19ステータスを確認するために電話でフォローアップされました。
Statistical analysis
Statistical analysis was done using STATA 13.0 software.
統計分析は、STATA13.0ソフトウェアを使用して行われました。
The mean and standard deviation was reported for continuous variables and proportions for categorical variables.
連続変数の平均と標準偏差、およびカテゴリ変数の比率が報告されました。
The log-binomial model was used to estimate adjusted relative risk.
対数二項モデルを使用して、調整された相対リスクを推定しました。
We also performed a sensitivity analysis, excluding those who were COVID-19 positive before the ivermectin prophylaxis.
また、イベルメクチン予防前にCOVID-19陽性であった人を除いて、感度分析を行いました。
Kaplan-Meier failure plot was used to estimate the probability of SARS-CoV-2 infectionwith follow-up time.
カプランマイヤー失敗プロットを使用して、フォローアップ時間とともにSARS-CoV-2感染の確率を推定しました。
Ethical consideration
The protocol was approved by the Institutional Ethics Committee of AIIMS Bhubaneswar (T/IMNF/CM&FM/20/142).
プロトコルは、AIIMSブバネシュワールの組織倫理委員会(T / IMNF / CM&FM / 20/142)によって承認されました。
Written informed consent was obtained from each participant.
各参加者から書面によるインフォームドコンセントが得られた。
Efforts were taken to maintain the anonymity of the participants throughout the process.
プロセス全体を通じて参加者の匿名性を維持するための努力が払われました。
COVID19 positive HCWs and students during the study period were treated at the institute.
研究期間中のCOVID19陽性の医療従事者と学生は研究所で治療を受けました。
Results
The institute was functioning with 3892 members during September 2020.
研究所は2020年9月に3892人のメンバーで機能していました。
Out of 3892, 262 were excluded from the study as they did not consent to participate in the study.
3892人のうち、262人は調査への参加に同意しなかったため、調査から除外されました。
Another 98 participants could not be followed up and were excluded from the study.
別の98人の参加者はフォローアップできず、調査から除外されました。
A total of 3532 participants were included in the study.
合計3532人の参加者が調査に含まれました。
The mean (SD) age was 30.6(8.6) years.
平均(SD)年齢は30.6(8.6)歳でした。
Over half of the study participants were less than 30 years (53.4%), while one-third (32.3%) were in the 30 to 39 years age group.
調査参加者の半数以上は30歳未満(53.4%)でしたが、3分の1(32.3%)は30〜39歳の年齢層でした。
The majority of participants were male (67.6%).
参加者の大多数は男性でした(67.6%)。
Approximately three-fourths (72.7%) of the participants were involved in the direct management of COVID-19 patients.
参加者の約4分の3(72.7%)が、COVID-19患者の直接管理に関与していました。
Administrative staff and students comprised 13.9% and 13.4%, respectively.
管理スタッフと学生はそれぞれ13.9%と13.4%を占めていました。
Among the 2567 participants, who were involved in COVID-19 patient care, 812 were doctors, 717 were nursing ocers, and 1038 were supporting staff. [Table 1]
COVID-19患者ケアに関与した2567人の参加者のうち、812人が医師、717人が看護師、1038人がサポートスタッフでした。 [表1]

Uptake of ivermectin was 67.5% (62.2% two-doses and 5.3% single-dose).
イベルメクチンの取り込みは67.5%でした(62.2%の2回投与と5.3%の単回投与)。
Rest 1147 (32.5%) participants did not consume ivermectin as prophylaxis.
残りの1147人(32.5%)の参加者は、予防としてイベルメクチンを摂取しませんでした。
The symptoms suggestive of SARS-CoV-2 infection(as per WHO guideline), were present among 331 (9.4%) participants during one-month follow-up.
SARS-CoV-2感染を示唆する症状(WHOガイドラインによる)は、1か月のフォローアップ中に331人(9.4%)の参加者に見られました。
A total of 201 (5.7%) persons within our cohort tested COVID-19 positive during the one-month follow-up period.[Table 1]
コホート内の合計201人(5.7%)が、1か月のフォローアップ期間中にCOVID-19陽性をテストしました。[表1]
Ivermectin prophylaxis uptake was better with increasing age and among males.
イベルメクチンの予防的摂取は、年齢が上がるにつれて、そして男性の間でより良くなりました。
Out of 331 participants, who had symptoms suggestive of SARS-CoV-2 infection, 200 (60.4%) participants were from the group who have not taken ivermectin prophylaxis.
SARS-CoV-2感染を示唆する症状を示した331人の参加者のうち、200人(60.4%)の参加者は、イベルメクチン予防を受けていないグループからのものでした。
The participants who took ivermectin prophylaxis had a lower risk of getting symptoms suggestive of SARS-CoV-2 infection(6% vs 15%). [Table 2]
イベルメクチン予防を行った参加者は、SARS-CoV-2感染を示唆する症状を示すリスクが低かった(6%対15%)。 【表2】

The incidence of SARS-CoV-2 infection was found lower in the ivermectin prophylaxis group compared to the group without ivermectin (2.0% vs 11.7%).
SARS-CoV-2感染の発生率は、イベルメクチンを投与していないグループと比較して、イベルメクチン予防グループの方が低いことがわかりました(2.0%対11.7%)。
The absolute risk reduction was 9.7%.
絶対的なリスク削減は9.7%でした。
Participants who had taken two-doses of ivermectin prophylaxis had a lower risk of contracting COVID-19 disease (RR0.18, 95% CI, 0.13-0.25) in the following month after receiving prophylaxis.
イベルメクチン予防を2回服用した参加者は、予防を受けた翌月にCOVID-19感染症にかかるリスクが低かった(RR0.18、95%CI、0.13-0.25)。
On adjusting for age, sex, and profession, the single-dose of ivermectin intake was not significant for lowering the risk of (ARR 1.04, 95% CI, 0.69-1.58).
年齢、性別、職業を調整したところ、イベルメクチンの単回投与はリスクを低下させるのに有意ではありませんでした(ARR 1.04、95%CI、0.69-1.58)。
However, two-doses of ivermectin prophylaxis had a significantly lower risk (ARR 0.17; 95% CI, 0.12-0.23).
ただし、イベルメクチン予防の2回投与では、リスクが大幅に低くなりました(ARR 0.17; 95%CI、0.12-0.23)。
Females had a lower risk of contracting COVID-19 disease compared to males (ARR 0.70 95% CI, 0.52-0.93). [Table 3]
女性は男性と比較してCOVID-19感染のリスクが低かった(ARR 0.70 95%CI、0.52-0.93)。 【表3】

We estimated the hazard ratio, excluding those who had been diagnosed as COVID-19 positive before the commencement of the study using the Kaplan-Meier method.
カプランマイヤー法を使用して、研究の開始前にCOVID-19陽性と診断された人を除いて、ハザード比を推定しました。
The probability of SARS-CoV-2 infectionwas 85% lower in those taking two-dose ivermectin at the end of 30 days (HR 0.15; 95% CI, 0.11-0.21). [Figure 1]
SARS-CoV-2感染の確率は、30日の終わりに2回投与のイベルメクチンを服用している人で85%低かった(HR 0.15; 95%CI、0.11-0.21)。
Information regarding adverse effects was collected through the existing pharmacovigilance services of the institute, and telephonic follow up.
副作用に関する情報は、研究所の既存のファーマコビジランスサービスと電話によるフォローアップを通じて収集されました。
A total of 42 (1.8%) participants reported adverse events following oral ivermectin.
合計42人(1.8%)の参加者が、経口イベルメクチンに続く有害事象を報告しました。
All adverse effects were self-limiting and mild in nature, and none required medication or hospitalization.
すべての副作用は自己制限的で軽度であり、投薬や入院は必要ありませんでした。
Adverse events were-headache, diarrhoea, nausea, itching, rashes, fatigue, vomiting, dizziness, and abdominal pain. [Table S1]
有害事象は、頭痛、下痢、吐き気、かゆみ、発疹、倦怠感、嘔吐、めまい、腹痛でした。
Discussion
We observed that the HCWs who took ivermectin chemoprophylaxis had an 83% lower risk of contracting COVID-19 disease in the following month compared to those who did not receive the drug.
イベルメクチンの化学的予防法を服用した医療従事者は、薬を服用しなかった医療従事者と比較して、翌月にCOVID-19感染症にかかるリスクが83%低いことがわかりました。
Based on its long history of clinical use, favourable safety prole, and emerging evidence from the in-vitro study, observationalstudy, and open-label RCT, ivermectin was used as a prophylactic agent for COVID-19 disease in our hospital for HCWs and has shown promising results.
臨床使用の長い歴史、好ましい安全性プロファイル、およびin vitro研究、観察研究、および非盲検RCTからの新たな証拠に基づいて、イベルメクチンは、当院の医療従事者向けのCOVID-19疾患の予防薬として使用されており、有望な結果を示しています。
The adverse effects reported by the subjects were few and t into the safety prole of this drug.
被験者から報告された副作用はほとんどなく、この薬の安全性プロファイルに影響を及ぼしました。
Ivermectin is a widely available anti-parasitic drug and has been included in the WHO list of essential medicines.
イベルメクチンは広く利用可能な抗寄生虫薬であり、WHO必須医薬品リストに含まれています。
The safety of the drug has been established by its large-scale use in the last four decades for various indications such as onchocerciasis, scabies, head lice, and other parasitic infestations such as ascariasis and trichuriasis.
この薬の安全性は、オンコセルカ症、疥癬、アタマジラミ、および回虫症や鞭虫症などの他の寄生虫感染症などのさまざまな適応症に対して、過去40年間に大規模に使用されたことによって確立されました。
Ivermectin has been reported to inhibit the interaction between importin (IMP) α/β1 heterodimer integrase protein, which helps in the nuclear import and propagation of infection by RNA viruses.
イベルメクチンは、インポーチン(IMP)α/β1ヘテロダイマーインテグラーゼタンパク質間の相互作用を阻害することが報告されています。これは、RNAウイルスによる感染の核移行と伝播に役立ちます。
It exerts its antiviral activity against a variety of RNA viruses, including West Nile virus, Inuenza virus, and Dengue virus.
ウエストナイルウイルス、イヌエンザウイルス、デング熱ウイルスなど、さまざまなRNAウイルスに対して抗ウイルス活性を発揮します。
An in-vitro study by Caly et al. reported a nearly 5000 fold reduction in the SARS-CoV-2 viral RNA with the use of ivermectin.
Calyらによるinvitro研究では、イベルメクチンを使用すると、SARS-CoV-2ウイルスRNAが5000分の1に減少することが報告されています。
However, a simulation study has suggested that despite a high lung: plasma concentration ratio, ivermectin would not achieve the required inhibitory concentration in the lungs after a single oral administration at the approved dose and may necessitate much higher doses.
ただし、シミュレーション研究によると、肺と血漿の濃度比が高いにもかかわらず、イベルメクチンは承認された用量での単回経口投与後に肺で必要な抑制濃度を達成できず、はるかに高い用量が必要になる可能性があります。
Nevertheless, clinical studies have shown that the addition of ivermectin at doses ranging from 150 to 200 μg/kg body weight led to lower mortality and greater clinical improvement in COVID-19 patients.
それにもかかわらず、臨床研究では、150〜200μg / kg体重の範囲の用量でイベルメクチンを追加すると、COVID-19患者の死亡率が低下し、臨床的改善が大きくなることが示されています。
A recent meta-analysis explored its therapeutic potential in COVID-19 patients and reported a signicant reduction in all-cause mortality with a pooled odds ratio of 0.53 (95%CI: 0.29 -0.96, p=0.04) with the addition of ivermectin as compared to standard therapy.
最近のメタアナリシスでは、COVID-19患者における治療の可能性を調査し、プールされたオッズ比0.53 (95%CI: 0.29 -0.96, p=0.04)ですべての原因による死亡率が大幅に減少したことを報告しました。標準治療と比較してイベルメクチンが追加されています。
A recent retrospective cohort study by Rajter JC et al. also demonstrated that ivermectin lowered mortality during treatment of COVID19.
Rajter JCらによる最近の後ろ向きコホート研究でも、イベルメクチンがCOVID19の治療中に死亡率を低下させることが示されました。
A randomized open-label clinical trial carried out by Shouman et al. in Egypt showed that prophylactic ivermectin therapy at an average dose of 300 μg/kg body weight in primary contacts of COVID-19 patients led to signicantly lower infections (7.4%) compared to controls (58.4%).
Shouman et alがエジプトで実施したランダム化非盲検臨床試験では、COVID-19患者の一次接触者に平均300μg/ kg体重の予防的イベルメクチン療法を行うと、コントロール群(58.4%)と比較して、感染症が大幅に減少した(7.4%)ことが示されました。
The half-life of the drug is 12-36 hours following oral administration, and it undergoes hepatic metabolism and is eliminated primarily through the faecal route over 12 days, with less than 1% being eliminated through the renal route.
薬物の半減期は経口投与後12〜36時間であり、肝代謝を受け、主に12日間にわたって糞便経路で排泄され、腎臓経路で排泄されるのは1%未満です。
The active metabolites persist in the body for three days.
活性代謝物は体内で3日間持続します。
The dose regimen chosen for prophylaxis in our study was thus based on these pharmacokinetic parameters, and the fact that dosage chosen in the clinical trial by Shouman was associated with high clinical efficacy and low rate of adverse events.
したがって、私たちの研究で予防のために選択された投与計画は、これらの薬物動態パラメータに基づいており、Shoumanによる臨床試験で選択された投与量は、高い臨床効果と低い有害事象の発生率に関連していました。
In our study, we also nd that females had a lower risk of SARS-CoV-2 infectioncompared to males.
私たちの研究では、男性と比較して女性の方がSARS-CoV-2感染のリスクが低いこともわかりました。
The previous research from India also had similar findings.
インドからの以前の研究でも同様の発見がありました。
The strengths of our study are the large sample size, minimal loss to follow-up, and the establishment of temporality.
私たちの研究の強みは、サンプルサイズが大きいこと、フォローアップの損失が最小限であること、および一時性の確立です。
The ideal study design to answer our research question would be a randomized controlled clinical trial.
リサーチクエスチョンに答える理想的な研究デザインは、ランダム化比較臨床試験です。
However, due to ethical reasons, we could not choose this design.
しかし、倫理的な理由から、このデザインを選択することはできませんでした。
HCWs who took ivermectin may somehow differ from the HCWs who did not prefer to take the prophylaxis in their behaviour.
イベルメクチンを服用した医療従事者は、予防措置をとることを好まなかった医療従事者とはどういうわけか異なる可能性があります。
However, we had a strong institutional policy in place related to COVID-19 appropriate behaviour in the workplace, which may have avoided the possible bias.
ただし、職場でのCOVID-19の適切な行動に関連する強力な制度的ポリシーがあり、バイアスの可能性を回避できた可能性があります。
The major limitation is that we only tested HCWs who either developed symptoms or who were direct or high-risk contacts of positive patients.
主な制限は、症状が現れた、または陽性患者の直接または高リスクの接触者であった医療従事者のみをテストしたことです。
This was done in keeping with the Government strategy for COVID-19 testing in India.
これは、インドでのCOVID-19テストに関する政府の戦略に沿って行われました。
However, this precludes us from including the HCWs who may have been asymptomatic or mildly symptomatic and chose not to get tested.
ただし、これにより、無症候性または軽度の症候性であり、検査を受けないことを選択した医療従事者を含めることができなくなります。
This may be a small number, but the interpretation of our results must also take this factor into account.
これは少数かもしれませんが、結果の解釈ではこの要素も考慮に入れる必要があります。
We believe that ivermectin is a low-cost prophylaxis that can easily be used in many settings to reduce the burden of the disease until a vaccine is successfully rolled out widely.
イベルメクチンは低コストの予防法であり、ワクチンが広く普及するまで、さまざまな状況で簡単に使用して病気の負担を軽減できると考えています。
Further research is required to guide the frequency of chemoprevention, acceptability, and cost-effectiveness in the community setting.
コミュニティ環境での化学的予防の頻度、受容性、費用対効果を導くには、さらなる研究が必要です。
Conclusion
In addition to behaviour prophylaxis, two-doses (300 μg/kg at a gap of 72 hours) of ivermectin chemoprophylaxis reduces COVID-19 disease by 83% among healthcare workers for one month.
行動の予防に加えて、イベルメクチンの化学的予防の2回投与(72時間のギャップで300μg/ kg)は、医療従事者のCOVID-19疾患を1か月間83%減少させます。
Ivermectin is safe and may constitute a cost-effective strategy to prevent COVID-19 disease until a vaccine is available for general use.
イベルメクチンは安全であり、ワクチンが一般的に使用できるようになるまでCOVID-19病を予防するための費用効果の高い戦略となる可能性があります。
Further research is required to guide the frequency of chemoprevention, acceptability, and cost-effectiveness in the community setting.
コミュニティ環境における化学的予防の頻度、受容性、費用対効果を導くには、さらなる研究が必要です。
以下省略。
この記事が気に入ったらサポートをしてみませんか?