
109 骨壊死

キーポイント
・大腿骨頭は骨壊死の最も一般的な部位である。
・ 副腎皮質ステロイドは非外傷性骨壊死の最も一般的な原因である。
・まれに、顎骨壊死がビスフォスフォネート製剤の投与と関連することがある。この現象は、ビスフォスフォネート製剤の点滴静注を繰り返した場合に多くみられる。
・デノスマブなど他の薬剤と関連した顎骨壊死の症例も報告されている。 若年患者は変形性関節症よりも骨壊死に罹患することが多く、骨壊死の長期罹患率は有意に高い。
・脂質代謝異常、骨ホメオスタシス異常、アポトーシス制御異常、凝固異常、自然免疫異常、酸化ストレス異常が骨壊死の病因に関与している可能性がある。
・骨壊死の病態に共通する最後の経路は、骨片への血液供給の途絶である。
・MRIは現在、早期診断と骨壊死の範囲の同定に最適な検査である。
・大腿骨頭壊死症の外科的治療には多くのバリエーションがあるが、症状のある患者のほとんどは最終的に人工股関節全置換術を必要とする。
・骨壊死の管理を成功させるためには、危険因子の知識と早期発見が重要である。
Pearl:骨壊死という病態を表す用語はこれまでの歴史で様々な用語が使用されている
Comment: Osteonecrosis means “bone death” (ossis [Latin] = bone; necrosis = killing or causing to die). Synonyms include avascular necrosis, ischemic necrosis of bone, aseptic necrosis, and subchondral avascular necrosis. Although the term osteonecrosis dissecans is sometimes used, it is actually a consequence of osteonecrosis involving fragmentation of bone that leads to fracturing or cracking of bone. The concept of bone death was first described by Hippocrates,1 but the first clinical description of osteonecrosis was a case of sepsis-induced bone death described by Russell in 1794. The first description of the occurrence of bone death in the absence of infection was published almost a century later. The first report of osteonecrosis in a deep sea diver appeared in 1936.
・骨壊死とは「骨の死」を意味する(ossis[ラテン語]=骨、necrosis=殺す、死に至らしめる)
・類義語には、avascular necrosis; 血管壊死、ischemic necrosis of bone; 虚血性骨壊死、aseptic necrosis; 無菌性壊死、subchondral avascular necrosis; 軟骨下血管壊死などがある。
・osteonecrosis dissecans; 離断性骨壊死という用語が使われることもあるが、この病名は骨折やひび割れにつながる骨の断片化を伴う骨壊死の結果である。
・骨壊死の概念はヒポクラテスによって最初に記述された。
・骨壊死の最初の臨床的記述は1794年にラッセルによって記述された敗血症誘発性骨死の症例であった。
・感染症を伴わない骨死の発生に関する最初の記述は、ほぼ1世紀後に発表された。深海潜水士における骨壊死の最初の報告は1936年に発表された。
Myth: 骨壊死は女性に多い
Reality: Osteonecrosis primarily affects men, except when associated with systemic lupus erythematosus.
・骨壊死は、全身性エリテマトーデスに伴う場合を除き、主に男性に発症する。
・SLEに多いイメージはあったので、ついつい女性に多いと思いがちですが、SLE以外では主に男性に生じるようです
・UpToDateによれば、アルコールに起因するものは男性に、SLEに関連するものは女性に多い、と記載があります(https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-osteonecrosis-avascular-necrosis-of-bone?search=oteonecrosis&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1#H256491200)
・30〜50歳代に好発することもおさえておきたいところです。
Pearl:骨壊死は様々な疾患との関連がありそうである
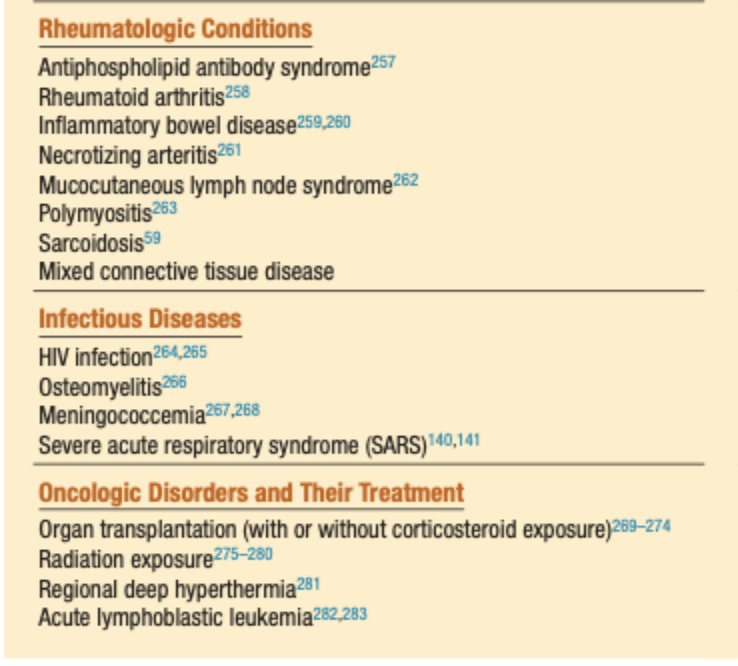
Comment: Osteonecrosis has been linked to numerous conditions. The evidence for a causal relationship varies greatly, and in some cases only case reports have been published. The most common cause of nontraumatic osteonecrosis is corticosteroid use, which was first described in 1957. Osteonecrosis has also been associated with metabolic disorders and pregnancy. Diagnosis is often delayed in mothers until months after delivery. Women who experience osteonecrosis during pregnancy tend to have a small body frame and a large weight gain.
・骨壊死は多くの疾患と関連している。
・因果関係を示す証拠は様々であり、症例報告のみが発表されている場合もある。非外傷性骨壊死の最も一般的な原因は、コルチコステロイドの使用であり、1957年に初めて報告された。
・骨壊死はまた、代謝異常や妊娠とも関連している。診断が遅れるのは、出産後数ヵ月経ってからである。妊娠中に骨壊死を経験する女性は、小柄で体重増加が大きい傾向がある。
・自分が勉強になったのは、代謝性疾患との関連です。
上記表を抜粋したものになります。

Myth:骨壊死を予防するための安全な糖質コルチコイド量にはある程度目安がある
Reality: Studies have been performed to determine the duration of use and the dosages of corticosteroids necessary to precipitate osteonecrosis. Because several forms of corticosteroids exist with differing potencies and half-lives, and because dosages and duration of use vary between studies, no conclusions about a “safe” dose of corticosteroids can be made.
・ 骨壊死を誘発するのに必要な副腎皮質ステロイドの使用期間と用量を決定するための研究が行われてきた。
・コルチコステロイドには効能や半減期が異なるものがいくつか存在し、使用量や使用期間も研究によって異なるため、コルチコステロイドの「安全な」使用量についての結論は出せない。
・Clin Rheumatol. 2002 Aug;21(4):299-303.
MRIでステージ1のosteonecrosis (ON)を生じた20人を検討
GC使用から診断までは1~16ヶ月, GC累積投与量は平均PSL換算5928mg
・Steroid induced osteonecrosis: An analysis of steroid dosing risk, Autoimmun Rev . 2010 Sep;9(11):721-43.
ポイント→投与量に依存, 長時間作用型ステロイドや非経口投与でリスク↑
SLEにおいてはCushing habitusと骨壊死に関連あり
1978年まではGCの使用とONは負の相関がある、とされていたが、1960年にDeboisが歴史上初めてONとGCの関連を指摘
・吸入や外用のステロイドはおそらくONとの関連なし
・骨壊死を起こしたときのステロイド量はあまり関係ない、少量でも起きる
治療開始して3ヶ月くらい、晩期合併症ではない
・大腿骨頭壊死だと思ったら、骨原発リンパ腫だった…なんて症例がありましたと、滝澤先生が教えてくれました。
Myths:大腿骨頭壊死が両側性となることは極めて稀である
Reality: The risk of developing osteonecrosis of the contralateral hip when one side is affected ranges from 31% to 55%.
・片側の股関節が侵された場合、反対側の股関節に骨壊死が生じるリスクは31%から55%である。
Myth:骨髄浮腫症候群は骨壊死の前段階と考えられている
Comment: A specific syndrome known as bone marrow edema syndrome was initially thought to be a precursor to osteonecrosis, but it is now believed to be a separate entity.
・骨髄浮腫症候群として知られる特殊な症候群は、当初は骨壊死の前駆症状であると考えられていたが、現在では別の疾患であると考えられている。
・骨髄浮腫の所見は骨壊死における一般的な所見であるが、特異的な所見ではないようです。骨髄炎、変形性関節症、潜因性骨内骨折、ストレス骨折、骨粗鬆症、鎌状赤血球症など、多くの筋骨格系疾患でみられる所見です。
・以前は”bone marrow edema syndrome”は骨壊死の前駆症状と考えられていたようですが. 現在は別の病気と考えられています。
・中年男性、妊娠第3期の女性に見られるもので、一過性・self-limittingな病態です。
・1ヶ月の初期相、1〜2ヶ月のプラトー相、さらに4〜6ヶ月の退行相があります。
・病理学的にはびまん性の間質性浮腫、脂肪骨髄細胞の断片化、および新生骨の形成増加などの所見がみられます。
・MRIである程度鑑別ができるようですが、説明が難しいです…
※骨髄浮腫症候群と骨壊死との鑑別は、動的造影3次元MRIに基づく平均通過時間 (MTT)や血漿流(PF)などの灌流パターンの解析によって容易になる。骨髄浮腫では、PFが高くMTTが低い軟骨下領域を、PFが低くMTTが長い領域が取り囲んでいる。対照的に、骨壊死では、PFとMTTのない軟骨下領域を、PFが高くMTTが中間の縁が取り囲んでいる。
Pearl:骨粗鬆症の治療薬であるビスホスホネート製剤、デノスマブ、ラロキシフェンでONJが報告されている。
Comment: Bisphosphonate-induced osteonecrosis of the jaw is particularly interesting because the intended beneficial use of bisphosphonates to treat osteoporosis and related disorders of bone formation instead leads to a serious bone complication. Two forms of bisphosphonates are available, and osteonecrosis appears to occur in association with bisphosphonates that contain nitrogen. The mechanism of bisphosphonate-induced ONJ appears to parallel that of glucocorticoids, with derangement in lipid metabolism, bone homeostasis, and apoptosis of bone cells all playing a role. Interestingly, the jawbone appears to be the most vulnerable bone in bisphosphonate-induced disease, as opposed to the femoral head. This phenomenon may be a result of the high bone turnover rate in the jaw or because bisphosphonates exert their action not only on bone but also on many elements of the surrounding tissue, including fibroblasts and blood vessels.
ONJ is increasingly recognized as a significant disease, and in addition to bisphosphonate use, other causes have been implicated. Many of these are case reports, but epidemiologic studies are beginning to appear. A case of ONJ was reported in association with the use of raloxifene. Raloxifene is a nonsteroidal benzothiophene that is used as an estrogen receptor modulator to treat osteoporosis in post-menopausal women and to reduce the risk of breast cancer. Denosumab, a monoclonal antibody against receptor activator of nuclear factor-κB ligand (RANKL) used in the treatment of osteoporosis, has also been implicated in ONJ. In addition to case reports,78–80 animal studies also suggest that anti-RANKL interferes with the normal bone resorptive functions of osteoclasts after dental trauma,which may play a role in the pathogenesis of ONJ.
・ビスフォスフォネート誘導性顎骨壊死は、骨粗鬆症とそれに関連する骨形成障害の治療にビスフォスフォネートを使用することが意図されているため、特に興味深い。2種類のビスフォスフォネートが使用可能であり、骨壊死は窒素を含むビスフォスフォネートに関連して起こるようである。
・ビスフォスフォネートによるONJの機序は、グルココルチコイドによるものと類似しているようで、脂質代謝の異常、骨恒常性の異常、骨細胞のアポトーシスがすべて関与している。興味深いことに、ビスフォスフォネート誘発性疾患では、大腿骨頭とは対照的に、顎骨が最も脆弱な骨であるようである。この現象は、顎の骨回転率が高いためか、ビスフォスフォネートが骨だけでなく、線維芽細胞や血管を含む周辺組織の多くの要素にも作用を及ぼすためであろう。
・ONJは重要な疾患として認識されるようになってきており、ビスフォスフォネート製剤の使用に加え、他の原因も示唆されている。これらの多くは症例報告であるが、疫学的研究も始まっている。ラロキシフェンの使用に関連してONJの症例が報告された。ラロキシフェンは非ステロイド性ベンゾチオフェンであり、エストロゲン受容体モジュレーターとして閉経後女性の骨粗鬆症治療や乳癌リスク軽減に使用されている。デノスマブは、骨粗鬆症の治療に使用される核因子-κBリガンド(RANKL)受容体活性化因子に対するモノクローナル抗体であるが、ONJとの関連も指摘されている。症例報告に加え、78-80の動物実験でも、抗RANKLが歯科外傷後の破骨細胞の正常な骨吸収機能を阻害することが示唆されており、これがONJの発症に関与している可能性がある。
・窒素を含むビスホスホネート製剤はアレンドロン酸、リセドロン酸、ゾレドロン酸で、窒素非含有なのはエチドロン酸のようです
・J Med Case Rep. 2011 Sep 23:5:477には、非がん患者に窒素含有のBPであるゾレドロン酸を年に1回投与しONJを発症と書いてありました。
・ラロキシフェンについては、Quintessence Int. 2015 May;46(5):423-8.の一例報告が引用されています。
・皆様御存知の通り、最もリスクが高いのはがん患者のゾレドロン酸です。
Pearl:大腿骨頭壊死の診断には本邦の厚生労働省の基準が用いられる。
Comment: In 2001 the Japanese Ministry of Health, Labor, and Welfare proposed revising criteria for the diagnosis and staging of osteonecrosis of the femoral head.109 Diagnostic criteria included (1) collapse of the femoral head without joint space narrowing or acetabular abnormality as seen on a plain radiograph, (2) demarcating scleosis in the femoral head without joint space narrowing or acetabular abnormality, (3) “cold in hot” areas on bone scans, (4) a low-intensity band on T1-weighted MRI, and (5) histologic findings of trabecular and marrow necrosis. If a patient fulfills two of the five criteria, the diagnosis is established.
・2001年厚生労働省は、大腿骨頭壊死症の診断と病期分類に関する基準の改訂を発表した。
診断基準には
(1)単純X線写真で関節腔の狭小化や寛骨臼の異常を伴わない大腿骨頭の虚脱
(2)関節腔の狭小化や寛骨臼の異常を伴わない大腿骨頭の境界明瞭な骨梁
(3)骨スキャンで”cold and hot”
(4)T1強調MRIで低強度帯
(5)組織学的に海綿体壊死と骨髄壊死が認められること、が含まれる。
患者が5つの基準のうち2つを満たせば、診断が確定する。
Pearl:大腿骨頭壊死のメカニズムは心臓における”冠動脈疾患”になぞらえられる
Comments: Osteonecrosis secondary to trauma can be easily explained simply based on anatomy, but with nontraumatic osteonecrosis, the pathogenesis is more complex and may involve immunologic, hormonal, and metabolic factors.The immunologic changes occurring in nontraumatic osteonecrosis may help explain why corticosteroids are particularly dangerous to the integrity of the blood supply of the femoral hip. Some investigators have likened osteonecrosis to “coronary disease” of the hip and propose that the same mechanisms that cause ischemia of the myocardium may also cause ischemia of the femoral head.
・非外傷性骨壊死で起こる免疫学的変化は、副腎皮質ステロイドが大腿骨股関節の血液供給の完全性にとって特に危険である理由を説明するのに役立つかもしれない。一部の研究者は、骨壊死を股関節の「冠動脈疾患」になぞらえ、心筋の虚血を引き起こすのと同じメカニズムが大腿骨頭の虚血も引き起こすと提唱している。

とはいうものの、それが何を意味しているのか、ちょっとよくわかりませんでした。
・ペルテス病では静脈還流が阻害され、骨内圧・関節内圧の上昇が観察されれています。
・損傷や炎症によって血管が変化すると、最終的に出血性梗塞につながることもあるようです。実際の大腿骨頭壊死の検体をみてみると、出血性梗塞の所見がしばしば見られるようでした。
Pearls:大腿骨頭壊死患者ではeNOSやプラスミノーゲン活性化因子インヒビター1(PAI-1)遺伝子の変異を有している場合が多い
Comments: Forty-one percent of patients with osteonecrosis compared with only 20% of controls were homozygous for the 4G/4G mutation in the plasminogen activator inhibitor-1 (PAI-1) gene.
・骨壊死と遺伝・環境要因の関連はまだよくわかっていません。
・一部のSNPsが骨壊死の発症と関連するという報告は多数見られます。
・その中でもeNOS(endothelial nitrix oxide synthetase; NO産生を促す酵素, NOは血管拡張を規定する重要なmediator)とPAI-1が注目されています。
・eNOS遺伝子のイントロン4におけるSNPsの解析では、ホモ4a対立遺伝子や4a/b対立遺伝子の頻度が、対照群と比較してすべてのタイプの骨壊死で高い、これらの遺伝子変異があるとeNOSのNO合成能力が低下しているケースが多く、NOが骨壊死に保護的に作用している可能性を示唆している
・骨壊死患者の41%がPAI-1遺伝子の4G/4Gホモ接合体を有しているという報告もあるようです。この変異は”低線溶性プラスミノーゲン活 性化因子インヒビター活性の上昇を引き起こし、その結果、刺激プラスミノーゲン活性 化因子活性が低下する”という減少を引き起こし、骨壊死の病態に寄与する、という病態が想定されています。
・それ以外にもVEGFのプロモーターやIL-23受容体の多型も骨壊死と関連している可能性があります。
Pearl:大腿骨頭壊死のMRI所見には特徴的なものがある
Comments: Currently, MRI is the gold standard for imaging of osteonecrosis. Most of the staging systems for osteonecrosis are now based on MRI appearance (Table 109.4). MRI of osteonecrosis can show changes earlier than conventional radiography or CT. It can also detect bone marrow edema, a feature sometimes seen in the early phases of osteonecrosis that is not visible on conventional radiography or CT.
The typical MRI findings in osteonecrosis are intermediate or low signal intensity on T1-weighted images and high signal intensity on T2-weighted and other water-sensitive sequences . As the disease progresses, the subchondral necrotic lesion is surrounded by a low signal line on T1-weighted images and a high signal line is seen on T2-weighted images, central to the low signal line, producing the (eFig. 109.2). MRI is performed in the sagittal, coronal, and axial planes and includes T1- and T2-weighted sequences. Although excellent correlation exists between histologic findings and MRI appearance (see Table 109.4), in most cases the necrotic area is composed of a variety of tissue, including areas of fibrosis and necrosis mixed with areas of blood and edema, depending on the age. Therefore the MRI signal of the necrotic area is often very heterogeneous (see Fig. 109.7), and as a result, this classification is of little clinical value. The low signal intensity band in the periphery of the osteonecrotic area correlates with a sclerotic band seen on radiographs and CT and often has a serpiginous appearance. When the osteonecrosis involves a long bone, this serpiginous band has been termed smoke in a chimney.“double-line” sign (Fig. 109.8). In advanced osteonecrosis, the necrotic segment exhibits low signal intensity on both T1-weighted and T2-weighted images.
・MRIは骨壊死の画像診断のゴールドスタンダードである。
・骨壊死の病期分類のほとんどはMRIの画像に基づいています。骨壊死のMRIは、従来のX線撮影やCTよりも早期に変化を示すことができます。

・骨壊死の典型的なMRI所見は、T1強調画像では中間または低信号強度、T2強調画像やその他の水感受性シーケンスでは高信号強度である。
・病態が進行すると、軟骨下壊死病変はT1強調像で低信号線に囲まれ、T2強調像では低信号線の中心に高信号線が認められ、"double-line "徴候が生じる(図109.8)。

・進行した骨壊死では、壊死部はT1強調像とT2強調像の両方で低信号強度を示す
・組織学的所見とMRIの外見には優れた相関があるが(上表 109.4参照)、ほとんどの場合、壊死部位は線維化部位や壊死部位に血液や浮腫が混在した部位など、年齢に応じてさまざまな 組織から構成されている。壊死領域のMRI信号は非常に不均一であることが多く、この分類はほとんど臨床的価値がない。
・骨壊死部周囲の低信号強度の帯は、レントゲン写真やCTでみられ る硬化帯と相関し、しばしば蛇紋岩(serpiginous band)のような外観を呈する。骨壊死が長骨に及んでいる場合、この蛇紋状の帯は”smoke in a chimney”(煙突の中の煙)と呼ばれている(図109.8)。
この記事が気に入ったらサポートをしてみませんか?