51 腰と膝の痛み

キーポイント
股関節痛や膝関節痛の鑑別診断は、病歴と身体診察で2~3種類に絞 ることができ、最終的に画像検査で診断を確定する。
最初の画像検査は、従来のX線写真を使用する。
膝の重要な構造の多くは、触診や誘発テストで簡単に調べることがで きる。
膝関節液貯留は多くの場合、内反症と関連している。
関節液貯留、関節包の圧痛、過伸展・過屈曲時の痛みがあれば、半月板断裂を疑 う。
変形性関節症の患者は、労作時にこわばりや痛みを訴えることが多い。
炎症性関節炎の場合、患者が関節を安静にしているにもかかわらず痛みを感じ続けていることが多い。
股関節の内旋に伴う鼠径部の痛みは、そうでないことが証明され るまでは、股関節疾患によるものと考えられる。
股関節疾患と腰仙部疾患の併発は一般的である。
はじめに
・股関節と膝関節は、筋・骨格系の痛みの最も多い部位の2つであり、60歳以上の股関節痛の有病率は8%から30%、55歳以上の膝関節痛の有 病率は20%から52%である。
・膝や股関節の痛みの報告を評価する際、鑑別診断のためには、これらの関節の解剖学的知識が必要である。
・膝の周囲は軟部組織が薄く、膝関節痛が他覚的に起こることはまれなため、病歴聴取と身体所見を十分に行うことで、膝関節痛の発生機序が明らかになることが多い。
・臀部痛の場合は、関節が深く、脊椎から痛みが伝 播することもまれではないため、 より困難なことが多い。
Pearls:膝関節痛の鑑別には年齢が重要な因子である
Comment: People in certain age groups tend to experience similar injuries. Ligament injuries, acute meniscus tears, and patellofemoral problems are frequently encountered in patients younger than 40 years. In contrast, degenerative conditions such as osteoarthritis and degenerative meniscal lesions tend to occur more frequently in older people.
・ある年齢層の人々は、同じような外傷を経験する傾向がある。
・靭帯損傷、急性の半月板断裂、膝蓋大腿障害は、40歳未満の患者に多く見られる。
・変形性関節症や退行性半月板損傷などの退行性疾患は、高齢者に多く見られる傾向があります。
Pearls:膝関節痛の診察では、患者に最も強い疼痛部位を指差ししてもらうこと、発生時期の確認が重要である
Comment: The patient should be able to point to the exact area where the pain is most severe. The time of onset of the pain should be determined.
・膝関節の構造の多くは皮下にあり、触診が容易である。
・膝は内側、外側、膝蓋大腿部の3つのコンパートメントに分けられる。各コンパートメントを別々に検査する。
・痛みが最も強い部位を正確に指し示す必要がある。
・痛みの発生時期も確認する。変形性関節症や炎症性関節炎は徐々に発症する傾向があるが、半月板や靭帯の損傷は通常外傷と関連している。例えば、膝を曲げた状態で負った損傷は半月板断裂を示唆するが、方向転換を伴う膝の非接触性損傷は前十字靭帯断裂の可能性が高い。
Pearls:膝関節痛の診察では、系統的にすべての膝の構造物を触診することが重要である
Comment: The examiner should then proceed with palpation of all structures of the knee. It is important to perform this palpation in a systematic manner to ensure completeness. Palpation should be gentle but firm enough to detect subtle disease. Structures to be palpated include the quadriceps tendon, the patella (superior and inferior poles), the pes anserinus bursa, the medial (Fig. 51.6A) and lateral (Fig. 51.6B) joint lines, the origins and insertions of the collateral ligaments, the tibial tubercle, and the popliteal fossa. Fullness in the posterior knee may be indicative of a Baker’s cyst.
・膝のすべての構造の触診を行う。この触診は系統的に行うことが重要である。
・触診すべき構造としては、大腿四頭筋腱、膝蓋骨(上極と下極)、鵞足包、内側関節線( 下図A)と外側関節線( 下図B)、側副靭帯の起始部と挿入部、脛骨結節、膝窩などがある。膝関節後面の膨隆は、Baker嚢胞の可能性がある。
Myth: 膝の不安定性には半月板損傷が最も寄与する
Reality: For example, the ACL is the primary restraint to anterior translation of the tibia, and the medial meniscus is the secondary restraint. ACL disruption will lead to a significant increase in anterior tibial translation. This translation will be increased if the patient has undergone a prior medial menisectomy.
・膝の安定性を決める要因にはprimary restraint(一次拘束)とsecondary restraint(二次拘束)がある。
・一次拘束が破壊されると、二次拘束によって運動が制限される
・二次拘束が損傷しても、一時拘束が無傷であれば運動には異常は生じない
・前十字靭帯(ACL)は脛骨の前方移動に対する一次拘束であり、内側半月板は二次拘束である。
・ACLが破壊されると、脛骨の前方移動が著しく増大する。患者が以前に内側半月板切除術を受けていれば、この前方移動はさらに増大する
Pearls:前十字靭帯損傷の診断に最も感度がよい検査は、前方引き出しテスト、Lachmanテスト、ピポットシフトテストである
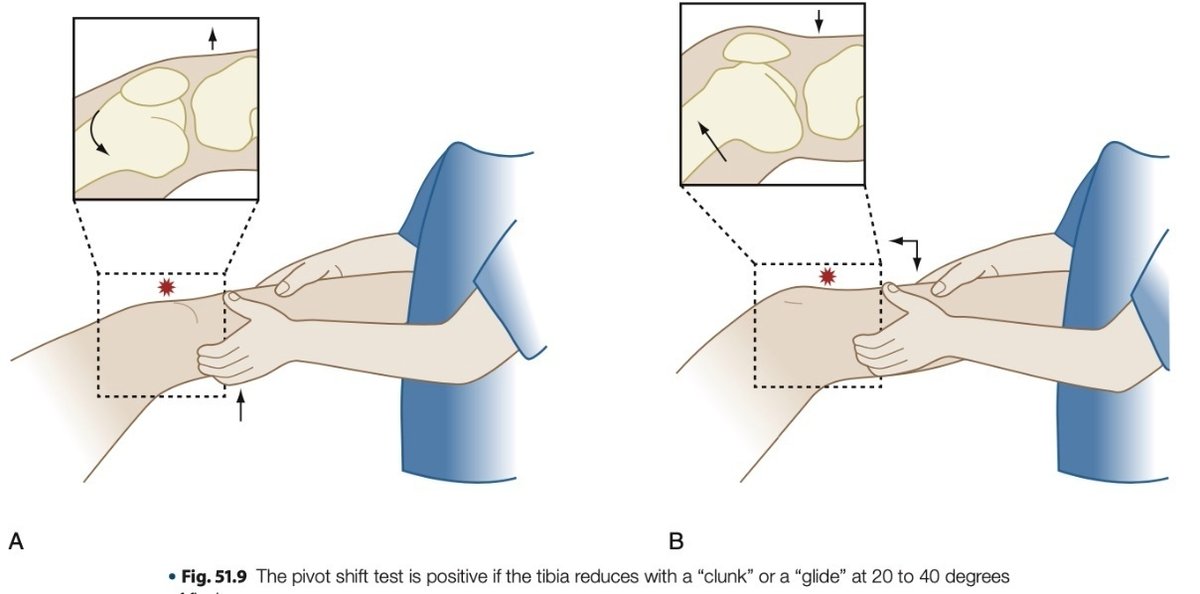
Comment: The most sensitive tests for diagnosis of an ACL injury include the anterior drawer, Lachman, and pivot-shift tests. All three tests are performed with the patient in the supine position. The anterior drawer test is performed with the knee flexed to 90 degrees. The examiner places his or her hands on the posterior surface of the proximal tibia and subluxates the tibia anteriorly. Any gross movement of the tibia that is different from the contralateral side is considered abnormal. The Lachman test is performed with the knee in 30 degrees of flexion (to remove the contribution of secondary restraints). The examiner applies an anterior force on the tibia while stabilizing the femur with his or her contralateral hand. Any increase in anterior tibial translation relative to the contralateral side is considered abnormal. The pivot-shift test is performed with the knee in extension. The examiner holds the tibia in slight internal rotation and applies a valgus stress while the knee is slowly flexed. This combination of forces should cause the tibia to subluxate anteriorly if the ACL is injured. The test is positive if the tibia reduces with a “clunk” or a “glide” at 20 to 40 degrees of flexion
・ACLは膝関節で最も頻繁に損傷する部位のひとつである。
・ACL不全は進行した変形性膝関節症の患者にもよくみられる。
・ACL損傷の診断に最も感度の高い検査は、前方引き出しテスト、Lachmanテスト、ピボットシフトテストである。
・これら3つの検査はすべて、患者を仰臥位にして行う。
・前方引き出しテストは、膝を90度に屈曲させた状態で行う。検査者は脛骨近位部の後面に手を置き、脛骨を前方に亜脱臼させる( 図51.7)。対側と異なる脛骨の肉眼的な動きは異常と判断する。

・Lachmanテストは、膝を30度屈曲させた状態で行う(二次的な 拘束の影響を取り除くため)。検査者は、対側の手で大腿骨を安定させながら、脛骨に前方への力を加える。対側に対して脛骨の前方移動が増加した場合は、異常と判断する。

・ピボットシフトテストは、膝を伸展位で行う。検査者は脛骨をわずかに内旋させた状態で保持し、膝をゆっくりと屈曲させながら外反ストレスをかける。ACLが損傷していれば、このような力の組み合わせによって脛骨が前方に亜脱臼するはずである。20~40度の屈曲で、脛骨が "カクン "または "グライド "するようであれば陽性である( 図51.9)。
・外反は文字通り外側に反らせる肢位です。X脚の肢位ですね。
・OA患者の痛みや膝の不安定性の原因にACL損傷が一定数隠れているかもしれません。ACL損傷見つけていきたいと思います。
Pearls:半月板損傷は外傷性・変形性ともに一般的な膝関節損傷の原因である
Comment: Traumatic and degenerative meniscal injuries are among the most common knee injuries.
・半月板断裂は通常、屈曲した膝が伸展に転じる際に起こる。
・内側半月板の断裂は外側半月板の断裂よりも一般的であるが、これは内側半月板が比較的可動性に乏しいためである。
・患者がよく訴えるのは、"ロッキング "や "カチッ "と いう音、あるいは膝が何かおかしいという感覚である。
・一般的な身体所見としては、過屈曲時および過伸展時の疼痛、関節包の圧痛、関節液貯留が挙げられる。
・半月板断裂の診断には、McMurrayテストやApley compressionテストは、感度や特異性に欠けるもののしばしば使用される。
・McMurrayテストは、患者を仰臥位にし、股関節と膝関節を90度まで屈曲させて行う。膝を屈曲位から伸展位へ動かす際に、膝に圧縮力と回旋力を加える。患者が痛みを訴えた場合、このテストは陽性となる

https://www.osmosis.org/learn/Special_tests_for_the_lower_limb
・Apley compression testは、患者をうつ伏せにし、膝を90度に屈曲させた状態で行う。検査が陽性であれば、患者は脛骨の回旋に伴う疼痛を訴える。

Pearls:大腿四頭筋腱損傷はSLEでしばしば見られる
Comment: njuries to the quadriceps tendon are most common in the sixth and seventh decades of life. Patients with systemic lupus erythematosus, renal failure, endocrinopathies, diabetes, and various other systemic inflammatory and metabolic diseases tend to be at a higher risk for these injuries.
・大腿四頭筋腱の損傷は、6~70年代に最も多くみられる。
・全身性エリテマトーデス、腎不全、内分泌病、糖尿病、その他様々な全身性の炎症性疾患や代謝性疾患を持つ患者は、これらの損傷のリスクが高い傾向がある。
・転倒やひねりによる損傷で大腿四頭筋の強烈な収縮を経験した後、強い膝前部痛を訴える。
・理学所見では、腱の欠損を触知するほか、血腫による関節液貯留、膝蓋骨の可動性亢進が認められる。患者は通常、膝を完全に伸ばすことができない
Pearls:股関節がぴきっと鳴る感覚は、snapping hip syndromeと呼ばれ、股関節内外のいくつかの障害で生じる
Comment: Patients occasionally report a “snapping” sensation in their hip. Extra-articular causes of hip snapping include a thickened iliotibial band snapping over the greater trochanter, the iliopsoas tendon gliding over the iliopectineal eminence, the long head of the biceps tendon rubbing on the ischial tuberosity, and the iliofemoral ligament rubbing on the femoral head. Intra-articular causes of snapping hip syndrome include loose bodies and large labral tears.
・股関節がスナッピングする関節外の原因:肥厚した腸脛靭帯が大転子の上でスナッピングする、腸骨棘腱が腸骨棘突起の上を滑走する、大腿二頭筋腱の長頭が坐骨結節を擦る、腸大腿靭帯が大腿骨頭を擦る、などが挙げられる。関節内原因には、ルーズボディや大きな臼蓋断裂などがある。
Myths:仙腸関節疾患はFABERテストで十分に診断可能である
Reality: Sacroiliac disease should be included in the differential diagnosis of hip pain. Although multiple provocative tests have been described to elicit sacroiliac disease, the FABER (flexion, abduction, and external rotation) test (also known as Patrick’s test) can help distinguish between hip and sacroiliac joint disease. With the patient supine, the clinician has the patient place his/her hip in the FABER position. The clinician then presses the flexed knee and the contralateral anterior superior iliac spine toward the floor. Pain in the buttocks suggests sacroiliac joint disease, whereas pain in the groin points to hip disease. If the sacroiliac joint is implicated, it is recommended that multiple other provocative tests be performed. Sacroiliac joint disease is the likely pain generator when three or more of the following tests are positive: the distraction, thigh thrust, compression, sacral thrust, Gaenslen’s, and FABER tests.
・仙腸関節疾患は、股関節痛の鑑別診断に含めるべきである。
・仙腸関節疾患を誘発する誘発テストは複数報告されているが、FABER(屈曲・外転・外旋)テスト(Patrick's testとしても知られる)は股関節疾患と仙腸関節疾患の鑑別に役立つ。
・FABERテストで仙腸関節が疑われる場合は、他の複数の誘発テストを行うことが推奨される。distraction test、大腿スラストテスト、圧迫テスト、仙骨スラストテスト、Gaenslen'sテスト、FABERテストのうち3つ以上が陽性であれば、仙腸関節疾患が痛みの原因である可能性が高い。

https://slideplayer.com/slide/17280353/

https://www.youtube.com/watch?app=desktop&v=DB3W2cWlA90
Myths:寛骨臼唇断裂は股関節痛の原因としては稀である
Reality: The acetabular labrum is drawing attention as a previously underappreciated cause of hip pain. Clinical presentation of a labral tear of the acetabulum may be variable, and the diagnosis is often delayed. Patients usually see multiple providers before the diagnosis is confirmed. In a series of 66 patients with arthroscopically confirmed tears of the acetabular labrum, 92% reported groin pain, 91% had activity-related pain, 71% reported pain at night, 86% described the pain as moderate to severe, and 95% had a positive impingement sign. The authors recommended that a diagnosis of acetabular labral tear be suspected in young, active patients reporting groin pain with or without trauma. The positive impingement test helps confirm the diagnosis of a labral tear. The test is positive if the patient experiences groin pain with the hip flexed, adducted, and internally rotated. The positive predictive value of this test ranges from 0.91 to 1.00 in six different studies.
・臼蓋唇(acetabular labrum)は、股関節痛の原因としてこれまで過小評価されてきたものとして注目されている。
・寛骨臼唇断裂(labral tear of the acetabulum) の臨床症状は様々で、診断が遅れることも多い。
・患者は通常、診断が確定するまでに複数の医療機関を受診する。関節鏡で寛骨臼の断裂が確認された66人の患者のシリーズでは、92%が鼡径部の痛み、91%が活動に関連した痛み、71%が夜間の痛み、86%が中等度から重度の痛み、95%がインピンジメント徴候陽性であった。
・著者らは、外傷の有無にかかわらず、鼡径部痛を訴える若く活動的な患者には、寛骨臼唇断裂の診断を疑うことを推奨している。
・インピンジメントテスト陽性は、臼蓋裂傷の診断確認に役立つ。このテストは、股関節を屈曲、内転、内旋させた状態で鼠径部の痛みがあれば陽性となる。このテストの陽性適中率は、6つの異なる研究で0.91~1.00であった。


左:前方インピンジメント 股関節を90度屈曲させ、強制的に内旋させるときに疼痛を誘発する
真ん中:前方のインピンジメントが強くなると、股関節屈曲時に自然と股関節が外旋してしまう(Drehamann’s sign)
右:後方インピンジメント 股関節を伸展させた状態で、股関節を外旋させる
J Child Orthop. 2012 Mar; 6(1): 1–12.
この記事が気に入ったらサポートをしてみませんか?