
78 シェーグレン症候群

キーポイント
・シェーグレン症候群は原発性または二次性で発症する。原発型は一般人口の0.06~1.5%にみられる。
・シェーグレン症候群の臨床的特徴は、乾燥性角結膜炎(ドライアイ)、口腔乾燥症(ドライマウス)、耳下腺の腫脹である。
・原発性シェーグレン症候群の腺外症状には、疲労、レイノー現象、多関節痛/関節炎、間質性肺疾患、神経障害、紫斑病などがある。
・涙腺および唾液腺への慢性単核球浸潤が特徴的な病理組織所見である。
・原発性シェーグレン症候群の診断は、ドライアイとドライマウスの主観的・客観的評価、血清抗核抗体検査、陰唇唾液腺生検によって行われる。
・シェーグレン症候群の治療は、現在、ドライアイとドライマウスの症状を緩和し、腺外症状をコントロールすることを目的としている。疾患修飾療法はまだ実験的である。
Pearl: 長らくミクリッツ病とシェーグレン症候群は類似した疾患と考えられていた
Comments: Because Sjögren’s cases were mostly middle-aged women, Morgan and Castleman incorrectly reasoned that Mikulicz’s disease was a subset of Sjögren’s syndrome with incomplete clinical manifestations. This now classic paper had the effect of unifying Mikulicz’s disease and Sjögren’s syndrome into a single disease entity.
・シェーグレンの症例はほとんどが中年女性であったため、MorganとCastlemanはミクリッツ病は不完全な臨床症状を示すシェーグレン症候群のサブセットであると誤って解釈した。今では古典となったこの論文は、ミクリッツ病とシェーグレン症候群を一つの疾患群に統一する効果をもたらした。
・シェーグレン症候群の歴史は19世紀に遡ります。
・1888年、Johann von Mikulicz-Radeckiは、涙腺、耳下腺、顎下腺の両側無痛性腫脹の症例を報告した。その後すぐに、ミクリッツ病は独立した病理学的なentitiyではなく、むしろ白血病、リンパ腫、結核によって引き起こされる臨床的ポプリ(”clinical potpourri”と原文で表現、臨床的特徴をもった寄せ集め、の意味?)であることを示す報告がなされた。
・1933年、スウェーデンの眼科医Henrik Sjögrenが、大唾液腺の腫脹を伴う2症例を含む19症例の角結膜炎を報告し、シェーグレン症候群の現代的な概念が定着した。
・1953年、MorganとCastlemanは、涙腺および唾液腺の腫大を有する18人の患者から得られた詳細な病理組織学的所見を発表した。 この病理学的論文は、Mikulicz病およびシェーグレン症候群に類似した臨床的特徴を有する症例で構成されていた。この古典的な論文は、ミクリッツ病とシェーグレン症候群を一つの疾患として統合する効果をもたらした。(A clinicopathologic study of Mikuliczs disease, Am J Pathol 29:579–580, 1953.)

・1960年12月2日、Joseph・J・Bunimがロンドンのヘバーデン演説(”Heberden Oration”)を行った際、彼は米国国立衛生研究所(NIH)の臨床センターで行ったシェーグレン症候群患者40人の臨床的、病理学的、検査検討についてエレガントに詳細に説明した。(Heberden Oration—a broader spectrum of sjogrens syndrome and its pathogenetic implications, Ann Rheum Dis 20:1–&, 1961.)

・彼らのシリーズに含まれるすべての患者は、以下の3つの特徴のうち少なくとも2つを有していた:sicca性角結膜炎、口腔乾燥症(唾液腺の腫大を伴うか伴わない)、関節リウマチ。
・NIHの症例の中で、TalalとBunimは、reticulum cell sarcoma(非ホジキンリンパ腫を含む古い用語)の患者3人と、ワルデンストレーム・マクログロブリン血症の患者4人に注目し、この疾患におけるリンパ腫のリスク上昇に初めて注目した。 彼らは、「慢性的な免疫亢進状態と異常な組織抗体を産生する免疫担当細胞の増殖が、悪性リンパ腫を比較的頻繁に発症させる素因になっている」と推測した。(The development of malignant lymphoma in the course of Sjoegren’s syndrome, Am J Med 36:529–540, 1964.)
・1965年、彼らは、他の結合組織疾患を伴わず、sicca症状を呈する患者16人のうち12人(75%)が、ラットの肝組織を用いた間接免疫蛍光法で血清抗核抗体(ANA)反応性が陽性であったと報告した(Antinuclear and precipitating auto-antibodies in Sjogrens syndrome, Ann Rheum Dis 24:16, 1965.)。 さらに、Ouchterlonyプレート法を適用して、これらの患者の16人中13人(81%)の血清が、後にRo(SS-A)とLa(SS-B)と命名されることとなる自己抗原のSjDとSjTに対する沈殿抗体を含んでいることを示した。

・1960年代後半から1970年代前半にかけて、口唇唾液腺生検がシェーグレン症候群の診断検査として研究され、これらの組織標本における慢性炎症の程度に基づいた等級分類の開発につながった。
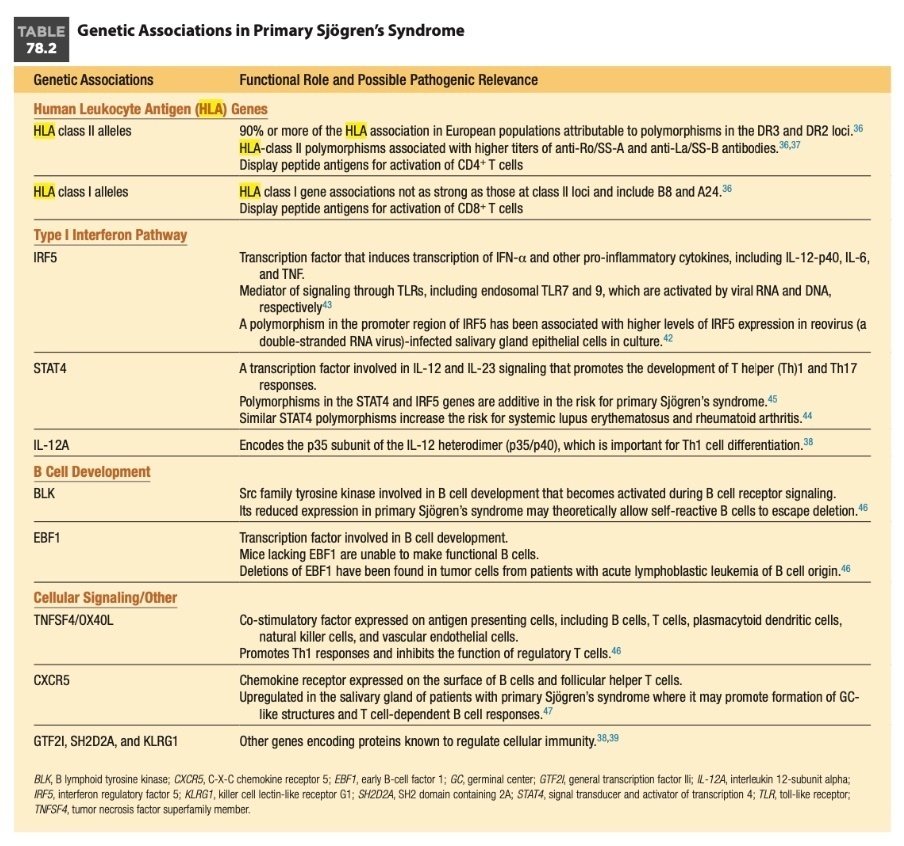
Pearl: 原発性シェーグレン症候群の疾患感受性に最も強く遺伝的に関与しているのは、ヒト染色体6p21上のHLA遺伝子、特にHLAクラスII対立遺伝子である。
Comments: The strongest genetic contributor to disease susceptibility in primary Sjögren’s syndrome can be found in the human leukocyte antigen (HLA) locus on human chromosome 6p21, especially the HLA-class II alleles.
・HLA以外のリスク対立遺伝子は、主にI型IFNシグナル伝達、B細胞発生、細胞性免疫に関連する遺伝子に存在することが示された。
・1型IFN経路の遺伝子は、原発性シェーグレン症候群患者の末梢血や唾液腺において、対照群と比較して高発現していることから、原発性シェーグレン症候群において特に注目されている。
・現在もSjogren症候群に対するanifrolumabの治験も走っているようです。
https://trialsearch.who.int/Trial2.aspx?TrialID=NCT05383677
Myths: 口唇生検で観察される浸潤細胞は単一なリンパ球の集団である
Reality: Studies of labial salivary gland biopsies from patients with primary Sjögren’s syndrome have shown approximately 90% of the infiltrating cells are CD4+ T lymphocytes and B lymphocytes, with the remainder an admixture of plasma cells, CD8+ T cells, FoxP3+ T regulatory cells, CD56+ natural killer (NK) cells, and macrophages, as well as myeloid and plasmacytoid dendritic cells (DCs).
・原発性シェーグレン症候群患者の口唇唾液腺生検の研究から、浸潤細胞の約90%がCD4+ Tリンパ球とBリンパ球であり、残りは形質細胞、CD8+ T細胞、FoxP3+ T制御細胞、CD56+ ナチュラルキラー(NK)細胞、マクロファージ、さらに骨髄性および形質細胞様樹状細胞(DC)が混在していることが示されている。


J Autoimmun. 2010 Jun;34(4):400-7.
・多彩な免疫細胞が口唇に浸潤しているのがわかりますね。唇でこんなに多様な免疫応答が起きていると思うと少しロマンがありますね。
・それ以外にも口唇生検の病理やサイトカインの検討では以下のような特徴があるようです。
①浸潤した単核球は、管や血管の周囲に集まる傾向があり、より重度の炎症性病変では、GC様構造に組織化された凝集塊を形成する。
②myeloid DCとマクロファージは、ほとんどが唾液管上皮に近接して存在し、TNF、IL-6、IL-10、IL-12、IL-18などの炎症性サイトカインを分泌する。
③小唾液腺はI型IFNの主要産生因子である形質細胞様DCを少数含んでいる。
④原発性シェーグレン症候群患者の唾液腺と末梢血には、強固な1型IFNシグネチャーが検出されている。
⑤原発性シェーグレン症候群患者の口唇唾液腺生検におけるT細胞サイトカインの解析は、主にTh1-およびTh17-主導型の反応を示唆している。原発性シェーグレン症候群の唾液腺微小環境は、トランスフォーミング増殖因子(TGF)-β、IL-6、IL-23にも富んでおり、これらはTh17細胞の発生を促進することが知られているサイトカインである
Myths: シェーグレン症候群ではムスカリン受容体に対する自己抗体が高率に検出される
Reality: The different assays for detecting serum anti-M3R antibodies in patients with primary Sjögren’s syndrome have produced inconsistent results. For this reason, it has been difficult to determine the diagnostic sensitivity and specificity of serum anti-M3R antibodies in primary Sjögren’s syndrome and the possible relationship of these autoantibodies to glandular hypofunction.
・ムスカリン受容体(MR)に対する自己抗体は、唾液腺機能障害を引き起こすというその役割の可能性から最も関心を集めている(ようです)。
・ムスカリン性3型受容体(M3)が原発性シェーグレン症候群における自己抗体の標的であるという仮説は以下に基づきます。①原発性シェーグレン症候群患者の血清免疫グロブリンは、腺房細胞膜上のM3R受容体に結合し、唾液腺細胞株におけるアセチルコリン誘発性Ca 2+応答を阻害する。 このCa 2+感受性反応は、先端膜のCl -チャネルを開き、浸透圧勾配と管腔への水の移動をもたらす細胞内シグナル伝達経路を通して、厳密に制御されている。②抗M3抗体の受動的移入は、シェーグレン症候群の動物モデルであるNODマウスにおいて腺機能低下を引き起こす可能性がある。
Pearl: 涙液膜の解剖学的構造はドライアイの鑑別診断に役立つ
Comments: The anatomy of the tear film informs the differential diagnosis of a dry eye (Table 78.4). The tear film consists of three major layers: the outer lipid layer, the middle aqueous layer, and the inner mucin layer. The middle aqueous layer is diminished in Sjögren’s syndrome. Conditions associated with infiltration of the lacrimal glands (e.g., sarcoidosis) and diminished tear flow (e.g., medications, aging, and estrogen deficiency) may also decrease aqueous tear flow. The lipid layer derives from the meibomian glands and traps the aqueous tear film on the eyeball and protects it from rapid evaporation. Meibomian gland dysfunction, or posterior blepharitis, produces dry eyes from rapid evaporation of tears; it often accompanies aqueous tear deficiency and can be an aggravating factor in patients with keratoconjunctivitis sicca that requires additional therapy. Meibomian gland dysfunction is often associated with ocular rosacea and seborrheic dermatitis, two conditions that also lead to dry eyes. Lipid degradation resulting from meibomian gland inflammation leads to the production of free fatty acids, which irritate the ocular surface and in turn may cause punctate keratopathy. The mucin layer originates from the goblet cells of the conjunctiva and, if deficient, leads to an uneven distribution of the tear film over the surface of the eye. Vitamin A deficiency and Stevens-Johnson syndrome are examples of conditions associated with an abnormal mucin layer.
・涙液膜は、外側の脂質層、中間房水層、内側のムチン層の3つの層から構成されている。シェーグレン症候群では中間房水層が減少している。
・涙腺の浸潤(サルコイドーシスなど)や涙液流量の減少(薬剤、加齢、エストロゲン欠乏症など)に関連する疾患も、涙液流量を減少させる可能性がある。
・脂質層はマイボーム腺に由来し、眼球上の涙液膜を捕捉し、急激な蒸発から保護する。
・マイボーム腺機能不全、または後眼瞼炎(posterior blepharitis)は、涙の急激な蒸発によるドライアイを生じさせる。これはしばしば涙液不足を伴い、さらに追加治療を必要とする瘢痕性角結膜炎患者の悪化因子となりうる。
・マイボーム腺機能不全は、ドライアイを引き起こす2つの疾患である眼酒さおよび脂漏性皮膚炎としばしば関連している。マイボーム腺の炎症に起因する脂質の分解は遊離脂肪酸の産生につながり、これが眼表面を刺激し、ひいては点状角膜症を引き起こすことがある。
・ムチン層は結膜の杯細胞に由来し、欠乏すると涙液が眼球表面に不均一に分布する。ビタミンA欠乏症やスティーブンス・ジョンソン症候群は、ムチン層の異常を伴う疾患の一例である。
・脂質はマイボーム腺から分泌
・水層とムチン層をターゲットした薬剤は存在している
https://www.youtube.com/watch?app=desktop&v=kTZQeij2WyY
https://brand.taisho.co.jp/iris/eye/dry-eye/001/
https://minds.jcqhc.or.jp/docs/gl_pdf/G0001116/4/dryeye_guideline.pdf
・SS 患者において涙液中の MUC5AC が健常人と比較して有意に減少している、というムチン産生の低下も関与、ジクアスやレバミピドはムチンを補う治療
Myths: シェーグレン症候群による有痛性の唾液腺腫脹はステロイド投与が必要となる場合が多い
Reality: Chronic swelling is usually painless and may be unilateral or bilateral; it is often diffuse and firm by palpation. Acute episodes of swelling are frequently painful and may intermittently punctuate the clinical course of primary Sjögren’s syndrome. These acute episodes, which likely result from dried mucus transiently obstructing the major ducts, usually subside within a few days with conservative therapy.
・原発性シェーグレン症候群患者の約4分の1が、疾患の経過中に耳下腺または顎下腺の腫大を来す。
・慢性の腫脹は通常無痛性で、片側性または両側性である。
・唾液腺腫脹の急性エピソードはしばしば疼痛を伴い、原発性シェーグレン症候群の臨床経過に断続的にみられることがある。急性のエピソードは、乾燥した粘液が一過性に大管を閉塞するために生じると考えられるが、通常は保存的治療により数日以内に治まる。
・まれに、細菌感染が急性の唾液腺腫脹を引き起こすことがあり、患者が発熱または他の体質的愁訴を有する場合は、可能性のある病因として考慮すべきである。
・増大する触知可能な硬結節を伴う非対称性腺腫大は、リンパ腫などの新生物を示すことがある。
Pearl: 原発性シェーグレン症候群の環状紅斑は、境界が隆起したドーナツリング様紅斑(I型)、わずかに鱗屑した多環状紅斑を伴う亜急性皮膚エリテマトーデス(SCLE)様の病変(II型)、および丘疹状の虫刺され様紅斑(III型)のいくつかの型があり、I型病変は原発性シェーグレン症候群に特異的で、欧米人ではなくアジア人に多くみられる。
Comments: Among the dermatologic manifestations of primary Sjögren’s syndrome, the most common are xerosis, or dry skin, eyelid dermatitis, and angular cheilitis. In addition, many patients develop a variety of other cutaneous manifestations, including annular erythema, purpura, and urticarial vasculitis. Annular erythema has been described in several forms: a donut-ring–like erythema with an elevated border (type I); a subacute cutaneous lupus erythematosus (SCLE)- like lesion with marginally scaled polycyclic erythema (type II); and a papular insect bite–like erythema (type III). Histopathologically, these lesions are characterized by a deep perivascular lymphocytic infiltrate without the epidermal changes associated with lupus.96 In some cases, immunoglobulin and complement deposition is observed along the basement membrane with liquefaction degeneration in the basal layer of the involved skin. The type I lesion appears to be specific for primary Sjögren’s syndrome, occurring predominantly in Asian as opposed to Western populations.
・原発性シェーグレン症候群の皮膚症状のうち、最も一般的なものは乾皮症、眼瞼皮膚炎および口角炎である。その他にも、環状紅斑、紫斑およびじんま疹性血管炎を含む他のさまざまな皮膚症状を発現する。
・環状紅斑は、境界が隆起したドーナツリング様紅斑(I型)、わずかに鱗屑した多環状紅斑を伴う亜急性皮膚エリテマトーデス(SCLE)様の病変(II型)、および丘疹状の虫刺され様紅斑(III型)のいくつかの型が報告されている(Dermatologica. 1977;154(2):115-27.
)。
・病理組織学的には表皮変化を伴わない深い血管周囲のリンパ球浸潤によって特徴づけられる。一部の症例では、免疫グロブリンと補体の沈着が基底膜に沿って観察され、皮膚基底層の液化変性がみられる。
・SLEに伴う環状紅斑の場合は、基底層の液状変性が特徴的ですが、シェーグレン症候群の場合は液状変性を起こしにくいとう記述もありました(Visual Dermatology_エリテマトーデスをきわめる_SLEエンサイクロペディア)。
Myths: ACPA陽性の原発性シェーグレン症候群の患者では関節リウマチの進行がよく見られる
Reality: In two separate studies, anti-citrullinated protein antibodies (ACPAs) were detected in serum from 7.5% and 9.9% of patients with primary Sjögren’s syndrome.100,101 However, in only one of these studies was their presence closely associated with synovitis,101 and in neither study did it appear that serum ACPA positivity was associated with radiographic erosions or progression to rheumatoid arthritis.
・2つの別々の研究(Prevalence of anti-cyclic citrullinated peptide and anti-keratin antibodies in patients with primary Sjogren’s syndrome, Ann Rheum Dis 64:114–117, 2005., Anti-cyclic citrul- linated peptide antibodies in primary Sjogren syndrome may be associated with non-erosive synovitis, Arthritis Res Ther 10:R51, 2008.)で、原発性シェーグレン症候群患者の7.5%と9.9%の血清から抗シトルリン化蛋白抗体(ACPA)が検出された。しかし、ACPAの存在が滑膜炎と密接に関連していたのは1つの研究のみであり、いずれの研究においても、血清ACPA陽性がX線写真上のびらんや関節リウマチへの進展と関連しているようには見えなかった。
・関節炎が先行するケースも原発性シェーグレン症候群ではしばしば見られます。
Pearl: 原発性シェーグレン症候群の糸球体病変は、腎臓における免疫複合体の沈着の結果であることが最も多く、尿細管間質性疾患よりもリンパ腫と関連することが多い。
Comments: Glomerular disease in primary Sjögren’s syndrome may take several forms, including membranous, mem- branoproliferative, mesangial proliferative, and focal crescentic glomerulonephritis. Glomerular disease is most often the result of immune complex deposition in the kidney and is more frequently associated with lymphoma than tubulointerstitial disease.
・原発性シェーグレン症候群における糸球体疾患は、膜性、膜増殖性、メサンギウム増殖性、および巣状半月体性糸球体腎炎を含むいくつかの形態をとりうる。糸球体病変は多くの場合、腎臓における免疫複合体の沈着の結果であり、尿細管間質性疾患よりもリンパ腫との関連性が高い(Clinically sig-nificant renal involvement in primary Sjogren’s syndrome: clini- cal presentation and outcome, Arthritis Rheum 65:2945–2953, 2013.)。
・免疫複合体がわんさか産生されて臓器障害を起こすタイプでは、リンパ腫のリスクが高い、というのは納得です。
Pearl: Schirmer検査は約20%の偽陰性率を示すが、眼異物感があるにもかかわらず涙液量が正常である場合は、眼瞼炎などの別の診断が示唆される。
Comments: Although a Schirmer-I test has an approximately 20% false-negative rate, normal tear flow in the face of ocular foreign body sensations suggests an alternative diagnosis such as blepharitis.
・各染色の特徴は以下のとおりです。
①リサミングリーン(結膜評価):ムチンを欠く上皮表面を染色
②フルオレセイン(角膜評価):眼球表面の細胞崩壊部位を染色するほか、涙液分解時間(BUT)の測定にも使用可能、BUT<10sだと、涙液の水層と脂質層の欠乏の両方の可能性を示唆する、よって涙腺が破壊されているのか、眼瞼炎(マイボーム腺の機能異常)を区別するかはできない
↑
上記2検査は2016年ACR/EULARの重要な構成要素
③ローズベンガル:変性もしくは死細胞の染色するが、角膜毒性があり最近は使用されない

Myths: 唾液腺シンチグラフィは原発性シェーグレン症候群の診断に対する感度特異度が優れた検査である
Reality: Scintigraphy is a radionuclide technique for measuring salivary gland function. After radiolabeled sodium pertechnetate technetium is injected into the blood, it is absorbed into the salivary gland and secreted into the mouth, allowing for determination of the salivary flow rate. The diagnostic sensitivity and specificity of salivary gland scintigraphy for the diagnosis of primary Sjögren’s syndrome has been estimated to be 75% and 78%, respectively.126 Salivary scintigraphy is not widely available for routine testing.
・放射性標識した過テクネチウム酸ナトリウムテクネチウムを血液中に注射した後、唾液腺に吸収され、口腔内に分泌されるため、唾液流量を測定することができる。
・原発性シェーグレン症候群の診断に対する唾液腺シンチグラフィーの診断感度および特異度は、それぞれ75%および78%と推定されている。
・唾液腺シンチグラフィは、ルーチンの検査として広く利用できるものではない(Assessment of salivary gland function in Sjogren’s syndrome: the role of salivary gland scintigraphy, Autoimmun Rev 8:672–676, 2009.)。
Myths: 口唇生検の解釈は評価者間での一致率が高い。
Reality: The interpretation of labial salivary gland biopsies is subject to considerable inter-reader variability, depending on the experience of the reader. Therefore, it is recommended that the biopsy slides be read by an experienced pathologist or other specialist with an appreciation for the nuances of interpretation.
・陰唇唾液腺生検の解釈は、読影者間でかなりのばらつきがある。したがって、生検スライドは、解釈のニュアンスを理解できる経験豊富な病理医またはその他の専門家が読影することが推奨される。
・解釈についてはKelley本文中に以下のような記載があります。
・生検の解釈に関する基本的なルールは、1994年にDanielsとWhitcherによって確立された。彼らは、lymphocytic fociはわずかな割合の形質細胞のみを含み、乳管拡張や線維化のない小葉の正常な小葉内腺房に隣接しているべきであると推奨している(Association of patterns of labial sali- vary-gland inflammation with keratoconjunctivitis sicca—analy- sis of 618 patients with suspected Sjogrens-syndrome, Arthritis Rheum-Us 37:869–877, 1994., Standardisation of labial salivary gland histopathology in clinical trials in primary Sjogren’s syndrome, Ann Rheum Dis 76:1161–1168, 2017.)。
・特に高齢者の生検標本の多くは、非特異的慢性唾液腺炎に一致する炎症パターン、すなわち、管拡張、腺房萎縮、線維化に伴うリンパ球と形質細胞の混合浸潤を示すため、これらのルールに従うことは重要である。慢性非特異性唾液腺炎をシェーグレン症候群と混同してはならない。
この記事が気に入ったらサポートをしてみませんか?