
COVID-19: Are there enough health workers? COVID-19症状に:医療従事者は十分に足りてますか?

As the COVID-19 crisis puts pressure on health services across the globe, ILOSTAT data highlights the already existing shortages of health workers. COVID-19発現危機は世界中の医療サービスにプレッシャーをかけているため、ILO(STAT)データは、既存の医療従事者の不足を浮き彫りにします。
The COVID-19 pandemic has brought countries’ health services into sharp focus. While governments move to slow the spread of the virus, health workers, especially women, are on the front lines of the epidemic.
In the face of this crisis, it’s reassuring to know that these workers are there to administer treatment and give advice. However, with more than half of the world’s population lacking access to essential health care, what happens when there aren’t enough doctors, nurses and support staff?
As part of the UN’s Sustainable Development Goals, all member states have agreed to achieve universal health coverage by 2030. With health employment density an indicator for this goal, an obstacle to its achievement is likely to be the shortage of health workers.
ILOSTAT data highlights the countries in greatest need. It presents the latest figures on skilled health occupations – such as doctors and nurses – and on general employment in the human health and social work sector, which includes all those employed in health-related establishments, including non-health occupations such as administrators and cleaners, and social work activities.
It shows that health is an important employment sector, but that countries’ capacities to recruit and retain health workers vary significantly across regions. This unequal distribution exacerbates inequities in access to health services.
COVID-19発現パンデミックにより、各国の医療サービスが注目されています。政府がウイルス(バーラス)のリクルートを遅らせるように動いている間、医療従事者、特に女性は流行のフロントラインにいます。
この危機に直面したとき、結果的に、そのワーカーが治療を管理し、助言することを知って安心します。しかし、世界の人口の半分以上が基本的なヘルスケアを利用できないため、十分な数の医師、看護師、サポートスタッフがいない場合はどうなりますか?
国連の持続可能な開発目標の一環として、すべての加盟国は2030年までに普遍的な医療保障(ユニバーサルヘルスケア)を達成することに同意しています。医療雇用密度はこの目標の指標であり、その達成への不平等は医療従事者の不足である可能性があります。
ILO(STAT)データは、最も必要としている国を強調しています。医師や看護師などの熟練した技術の職業と、管理者やクリーナーなどの健康を害する職業を含む、健康関連の施設で雇用されているすべての人を含む、人間の健康、ソーシャルワークセクターでの一般的な雇用に関する最新の数値を示します。 、ソーシャルワーク活動。
これは、健康が重要な雇用部門であることを示していますが、医療従事者を採用して維持する国の能力は、地域によって大きく異なります。この不平等な分配は、医療サービスへのアクセスの不平等を悪化させます。
Wealth and health
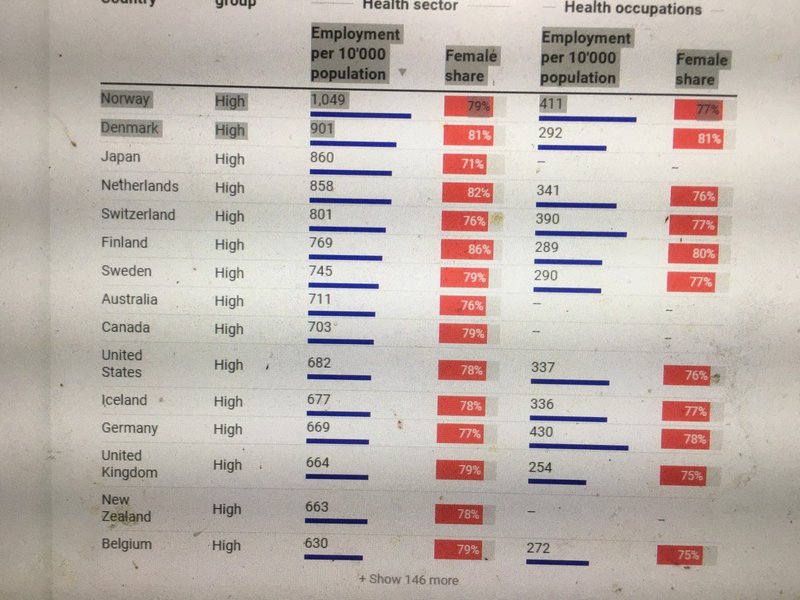
Health employment data (based on ISIC rev.4 category Q. Human health and social work activities) suggests that high-income countries have both the most skilled health workers and the largest health sectors relative to their population size. Norway has the largest health sector, employing 1,049 people per 10,000 population. Denmark, Japan, the Netherlands and Switzerland follow, all with over 800.
The US (682) and UK (664) have the 10th and 13th highest ratios respectively.
In fact, high-income countries collectively have nearly 12 times as many people employed in the health sector as low-income nations – 580 per 10,000 people compared with only 49.
Unequal access to health services
It’s a similar story when looking at skilled health occupations (such as doctors, nurses and midwives) per 10,000 people. Out of 97 countries with available data, the top 10 are almost exclusively high-income nations. Germany, Norway, Switzerland, the Netherlands and the US make up the top five, while the Russian Federation is the only non-high-income country in the top 10.
In many low-income countries, however, large parts of the population do not have access to essential health services due to the lack of health workers, particularly in rural and remote areas.
When the World Health Organization declared the COVID-19 outbreak a global health emergency, its greatest concern was the possibility of the virus spreading to countries with weaker health systems. In Africa, the average number of workers employed in the health sector per 10,000 people is 57. And many of the region’s poorer nations have far fewer.
富と健康
健康雇用データ(ISIC rev.4カテゴリQ.人間の健康とソーシャルワーク活動に基づく)は、高所得国に人口の大きさに対して最も熟練した医療従事者と最大の保健セクターの両方があることを示唆しています。ノルウェーは最大の保健セクターを有しており、人口10,000人あたり1,049人を雇用しています。デンマーク、日本、オランダ、スイスが続き、800人を超えています。
アメリカ(682)とイギリス(664)は、それぞれ10番目と13番目に高い比率です。
実際、高所得国の総人口は、低所得国の約12倍の人口であり、1万人あたり580人であるのに対し、49人だけです。
医療サービスへの不平等なアクセス
これは、1万人あたりの熟練した医療従事者(医師、看護師、助産師など)を見るときも同様です。利用可能なデータがある97か国のうち、上位10か国はほぼ独占的に高所得国です。トップ5はジャーマニー、ノルウェー、スイス、オランダ、アメリカであり、トップ10に入るのはロシアだけです。
しかし、多くの低所得国では、特に農村部や遠隔地の医療従事者が不足しているため、人口の大部分が不可欠な医療サービスを利用できません。
世界保健機関がCOVID-19発現を世界的な健康緊急事態と宣言したとき、その最大の懸念はウイルスがより弱い保健システムを持つ国に広がる可能性でした。アフリカでは、1万人あたりの医療部門で雇用されている労働者の平均数は57人です。この地域の貧しい国の多くは、はるかに少ない国です。
ILO modelled estimates for 2019 for the human health and social work sector (ISIC category Q), latest available national figures for skilled health occupations (ISCO categories 22 and 32) and UN estimates for population.
Source: ILOSTAT Get the data Created with Datawrapper
A critical factor in fighting pandemics
Even robust health systems can be severely tested by unexpected pressures such as the COVID-19 pandemic:
Of the 15 countries with the most confirmed reported COVID-19 cases to date, 14 of them have health employment data available in ILOSTAT. These data show that most of them (Austria, Belgium, Canada, France, Germany, Italy, Netherlands, Portugal, South Korea, Spain, Switzerland, United Kingdom and the United States) have well above the global average of 174 employed in the health sector per 10,000 people. In Iran, only 99 employed work in the health sector per 10,000 people, while there is no data on employment in the health sector available for China.
Having adequate numbers of health workers will be critical to winning the battle against COVID-19. But it is not the only issue. Access to personal protective equipment, occupational safety and health protocols, adequate rest and recovery periods and other working conditions will determine how effectively health workers can treat patients.
A predominantly female health workforce
Across the globe, added pressures could arise relating to the number of women working in healthcare. Globally, women make up 70% of those employed in the health sector and, based on data available for close to 100 countries, 72% of skilled health occupations. In short, women are disproportionately on the front lines in the world’s struggle to treat infected patients.
Meanwhile, women also carry the burden of unpaid care work, such as child rearing and care for the elderly. As schools close in regions affected by COVID-19, this creates additional challenges for many women health workers trying to balance work and family.
As the COVID-19 pandemic puts the world’s health services under the microscope, ILOSTAT data shows that numerous countries already faced shortages of health workers – often due to the long hours, low pay and occupational safety and health risks which deter many from entering the health workforce in the first place and which make many qualified health workers leave the profession prematurely.
To address the underlying reasons for these shortages, the ILO joined forces with the World Health Organization (WHO) and the Organisation for Economic Cooperation and Development (OECD) in the joint Working for Health Programme in 2017. Based on improved health labour market data, multi-stakeholder involvement, and social dialogue, this programme helps countries and constituents develop strategies to scale up investments in their health workforces.
パンデミック発現と闘いにおける重要な要素
頑丈なヘルスシステムでさえ、COVID-19発現パンデミックなどの予期しないプレッシャーによって厳しくテストされる可能性があります。
これまでに報告されたCOVID-19症例が最も確認されている15か国のうち、14か国がILO(STAT)で利用可能な医療雇用データを持っています。これらのデータは、ほとんどが(オーストリア、ベルギー、カナダ、フランス、ジャーマニー、イタリア、オランダ、ポルトガル、韓国(セウル)、スペイン、スイス、イギリス、アメリカ)が、健康に従事している174人の世界平均をはるかに上回っていることを示しています。 10,000人あたりのセクター。イランでは、10,000人あたり99人の保健医療従事者しか雇用されていませんが、中国で利用可能な保健医療従事者の雇用に関するデータはありません。
COVID-19発現と戦いに勝つには、適切な数の医療従事者がいることが重要です。しかし、それだけが問題ではありません。個人用保護具、労働安全衛生プロトコル、適切な休息、回復期間、その他の労働条件へのアクセスが、医療従事者が患者をいかに効果的に治療できるかを決定します。
主に女性の医療従事者(ナーシンング)
世界中で、ヘルスケアに従事する女性の数に関連して、追加プレッシャーが発生する可能性があります。世界的に、女性は健康分野で雇用されている女性の70%を占め、100か国近くで利用可能なデータに基づいて、熟練した健康な職業の72%を占めています。要するに、女性は感染した患者を治療するための世界の闘争のフロントラインに偏っています。
一方、女性は子育てや高齢者介護など、無給の介護(ケアテイカー)も担っています。 COVID-19発現影響を受ける地域で、学校が閉鎖されるにつれ、仕事と家族のバランスをとろうとする多くの女性医療従事者にさらなる課題をもたらします。
COVID-19発現パンデミックが世界の医療サービスを顕微鏡下に置くと、ILO(STAT)データは、多くの国がすでに多くの医療従事者の不足に直面していることを示しています。そもそも労働力が多く、多くの資格のある医療従事者が専門職を早々に辞めてしまう。
これらの不足の根本的な理由に対処するために、ILOは、2017年に共同で「保健医療プログラム」で世界保健機関(WHO)、経済協力開発機構(OECD)と力を合わせました。改善された医療労働市場データに基づいて、このプログラムは、複数の利害関係者の関与と社会的対話により、国と関係者が医療従事者への投資を拡大するための戦略を策定するのに役立ちます。
この記事が気に入ったらサポートをしてみませんか?